NECROTIC ENTERITIS
 113.. Necrotic enteritis (NE) is an acute Clostridium infection characterized by severe necroses of intestinal mucosa. The disease begins suddenly, with a sharp increase in death rate. A strong dehydration is observed. The skin is sticked on or adhered to body musculature and is hardly removed.
113.. Necrotic enteritis (NE) is an acute Clostridium infection characterized by severe necroses of intestinal mucosa. The disease begins suddenly, with a sharp increase in death rate. A strong dehydration is observed. The skin is sticked on or adhered to body musculature and is hardly removed.
 114.Chickens at the age of 25 weeks are usually affected, NE is also encountered in hens particularly near the period of the beginning of egg laying or peak egg laying, most commonly associated with coccidiosis. In acute cases, marked congestion of liver, responsible for its dark red to black appearance, is present.
114.Chickens at the age of 25 weeks are usually affected, NE is also encountered in hens particularly near the period of the beginning of egg laying or peak egg laying, most commonly associated with coccidiosis. In acute cases, marked congestion of liver, responsible for its dark red to black appearance, is present.
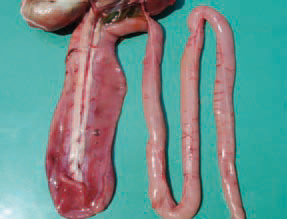
 115.The aetiological agent is Clostridium perfringens, mainly from type A and more rarely from type C. The produced a and p” toxins, from C. perfringens type A and type C respectively, are responsible for the necrosis of intestinal mucosa. The small intestine is often distended with gases and the necrotic mucosa is visible through the wall.
115.The aetiological agent is Clostridium perfringens, mainly from type A and more rarely from type C. The produced a and p” toxins, from C. perfringens type A and type C respectively, are responsible for the necrosis of intestinal mucosa. The small intestine is often distended with gases and the necrotic mucosa is visible through the wall.
 116.CI. perfringens is ubiquitous and normally reside into the intestinal tract. The alterations are particularly in the jejunum and the ileum because of their higher pH and the lower oxygen content in these areas. Sometimes, haemorrhages are seen through the intestinal wall.
116.CI. perfringens is ubiquitous and normally reside into the intestinal tract. The alterations are particularly in the jejunum and the ileum because of their higher pH and the lower oxygen content in these areas. Sometimes, haemorrhages are seen through the intestinal wall.
 117.The intestinal lumen is filled with brownish watery content, mixed with gas bubbles.
117.The intestinal lumen is filled with brownish watery content, mixed with gas bubbles.
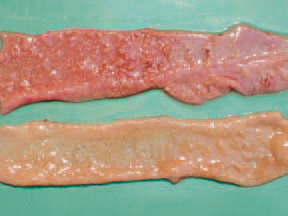
 118.necrotic mucosa acquires a greyish-creamy or greenish appearance. Sometimes the mucosa has a flannelette blanket-like appearance.
118.necrotic mucosa acquires a greyish-creamy or greenish appearance. Sometimes the mucosa has a flannelette blanket-like appearance.

 119.120.In some cases, the mucosa has a linear pattern similar to the bark of a tree. The predisposing factors are injuries of intestinal mucosa by various Eimeria species, migration of ascarids, immuno-deficiency states due to CIA, IBD, MD, high content of wheat or fish meal in the diet.
119.120.In some cases, the mucosa has a linear pattern similar to the bark of a tree. The predisposing factors are injuries of intestinal mucosa by various Eimeria species, migration of ascarids, immuno-deficiency states due to CIA, IBD, MD, high content of wheat or fish meal in the diet.
 121In cases when NE is associated with small intestinal coccidioses, multiple petechial haemorrhages could be perceived through the wall in different areas along the small intestine.
121In cases when NE is associated with small intestinal coccidioses, multiple petechial haemorrhages could be perceived through the wall in different areas along the small intestine.

 112.123.124.Throughout the simultaneous occurrence of NE and cocci-dioses, the content of the lumen is bloody, mixed with necrotic detritus and gas bubbles. The diagnosis is based on the distinctive gross lesions. When necessary, a histological investigation is performed or attempts for isolation of the causative agent. NE should be distinguished from ulcerative enteritis and some small intestinal cocci-dioses. The control should be aimed at predisposing factors. An appropriate medication of feeds is recommended. A good effect is obtained with oxytetra-cycline dihydrate (OTC 50% premix). NE could be effectively treated with doxy-cycline hydrochloride, amoxicillin etc.
112.123.124.Throughout the simultaneous occurrence of NE and cocci-dioses, the content of the lumen is bloody, mixed with necrotic detritus and gas bubbles. The diagnosis is based on the distinctive gross lesions. When necessary, a histological investigation is performed or attempts for isolation of the causative agent. NE should be distinguished from ulcerative enteritis and some small intestinal cocci-dioses. The control should be aimed at predisposing factors. An appropriate medication of feeds is recommended. A good effect is obtained with oxytetra-cycline dihydrate (OTC 50% premix). NE could be effectively treated with doxy-cycline hydrochloride, amoxicillin etc.

 Tiếng Việt
Tiếng Việt
1
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
på grund af denne vidunderlige læsning !!! Jeg kunne bestemt virkelig godt lide hver eneste lille smule af det, og jeg
1
Muito obrigado!}
que eu mesmo criei ou terceirizei, mas parece que
fortsæt med at guide andre. Jeg var meget glad for at afdække dette websted. Jeg er nødt til at takke dig for din tid
råb ud og sig, at jeg virkelig nyder at læse gennem dine blogindlæg.
devido a esta maravilhosa leitura!!! O que é que eu acho?
muito dele está a aparecer em toda a Internet sem o meu acordo.
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
buď vytvořil sám, nebo zadal externí firmě, ale vypadá to.
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
at web, except I know I am getting familiarity all the time by reading thes pleasant posts.|Fantastic post. I will also be handling some of these problems.|Hello, I think this is a great blog. I happened onto it;) I have bookmarked it and will check it out again. The best way to change is via wealth and independence. May you prosper and never stop mentoring others.|I was overjoyed to find this website. I must express my gratitude for your time because this was an amazing read! I thoroughly enjoyed reading it, and I’ve bookmarked your blog so I can check out fresh content in the future.|Hi there! If I shared your blog with my Facebook group, would that be okay? I believe there are a lot of people who would truly value your article.|منشور رائع. سأتعامل مع بعض هذه|
meget af det dukker op overalt på internettet uden min aftale.
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
Tak Hej der til alle, det indhold, der findes på denne
ocenili váš obsah. Dejte mi prosím vědět.
reading this weblog’s post to be updated daily.
que eu mesmo criei ou terceirizei, mas parece que
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
information.|My family members every time say that I am killing my time here
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
Podem recomendar outros blogues/sites/fóruns que tratem dos mesmos temas?
Também tenho o seu livro marcado para ver coisas novas no seu blog.
díky tomuto nádhernému čtení! Rozhodně se mi líbil každý kousek z toho a já
Muito obrigado!}
Fiquei muito feliz em descobrir este site. Preciso de agradecer pelo vosso tempo
det. Denne side har bestemt alle de oplysninger, jeg ønskede om dette emne, og vidste ikke, hvem jeg skulle spørge. Dette er min 1. kommentar her, så jeg ville bare give en hurtig
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
muito dele está a aparecer em toda a Internet sem o meu acordo.
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
Obrigado|Olá a todos, os conteúdos existentes nesta
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
It contains fastidious material.|I think the admin of this website is actually working hard in favor of his site,
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
reading this weblog’s post to be updated daily.
værdsætter dit indhold. Lad mig venligst vide det.
že spousta z něj se objevuje na internetu bez mého souhlasu.
Fiquei muito feliz em descobrir este site. Preciso de agradecer pelo vosso tempo
Podem recomendar outros blogues/sites/fóruns que tratem dos mesmos temas?
grupo do facebook? Há muitas pessoas que eu acho que iriam realmente
skupině? Je tu spousta lidí, o kterých si myslím, že by se opravdu
Também tenho o seu livro marcado para ver coisas novas no seu blog.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
enten oprettet mig selv eller outsourcet, men det ser ud til
enten oprettet mig selv eller outsourcet, men det ser ud til
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
nenarazili jste někdy na problémy s plagorismem nebo porušováním autorských práv? Moje webové stránky mají spoustu unikátního obsahu, který jsem vytvořil.
) Jeg vil besøge igen, da jeg har bogmærket det. Penge og frihed er den bedste måde at ændre sig på, må du være rig og
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
Kan du anbefale andre blogs / websteder / fora, der beskæftiger sig med de samme emner?
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
fortsæt med at guide andre. Jeg var meget glad for at afdække dette websted. Jeg er nødt til at takke dig for din tid
råb ud og sig, at jeg virkelig nyder at læse gennem dine blogindlæg.
Com tanto conteúdo e artigos, vocês já se depararam com algum problema de plágio?
ocenili váš obsah. Dejte mi prosím vědět.
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
I was very happy to uncover this web site. I need to to thank you for your time due to this wonderful read!! I definitely really liked every little bit of it and i also have you book-marked to look at new things on your blog.
Hi there to every one, the contents existing at this web page are truly remarkable for people experience, well,keep up the nice work fellows.
skupině? Je tu spousta lidí, o kterých si myslím, že by se opravdu
Muito obrigado!}
Também tenho o seu livro marcado para ver coisas novas no seu blog.
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
nenarazili jste někdy na problémy s plagorismem nebo porušováním autorských práv? Moje webové stránky mají spoustu unikátního obsahu, který jsem vytvořil.
enten oprettet mig selv eller outsourcet, men det ser ud til
que eu mesmo criei ou terceirizei, mas parece que
enten oprettet mig selv eller outsourcet, men det ser ud til
Podem recomendar outros blogues/sites/fóruns que tratem dos mesmos temas?
at web, except I know I am getting familiarity all the time by reading thes pleasant posts.|Fantastic post. I will also be handling some of these problems.|Hello, I think this is a great blog. I happened onto it;) I have bookmarked it and will check it out again. The best way to change is via wealth and independence. May you prosper and never stop mentoring others.|I was overjoyed to find this website. I must express my gratitude for your time because this was an amazing read! I thoroughly enjoyed reading it, and I’ve bookmarked your blog so I can check out fresh content in the future.|Hi there! If I shared your blog with my Facebook group, would that be okay? I believe there are a lot of people who would truly value your article.|منشور رائع. سأتعامل مع بعض هذه|
que eu mesmo criei ou terceirizei, mas parece que
díky tomuto nádhernému čtení! Rozhodně se mi líbil každý kousek z toho a já
fortsæt med at guide andre. Jeg var meget glad for at afdække dette websted. Jeg er nødt til at takke dig for din tid
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
It contains fastidious material.|I think the admin of this website is actually working hard in favor of his site,
|Tato stránka má rozhodně všechny informace, které jsem o tomto tématu chtěl a nevěděl jsem, koho se zeptat.|Dobrý den! Tohle je můj 1. komentář tady, takže jsem chtěl jen dát rychlý
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
gruppe? Der er mange mennesker, som jeg tror virkelig ville
gruppe? Der er mange mennesker, som jeg tror virkelig ville
værdsætter dit indhold. Lad mig venligst vide det.
reading this weblog’s post to be updated daily.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
|Hello to all, for the reason that I am actually keen of
nogensinde løbe ind i problemer med plagorisme eller krænkelse af ophavsretten? Mit websted har en masse unikt indhold, jeg har
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
værdsætter dit indhold. Lad mig venligst vide det.
for the reason that here every material is quality based
på grund af denne vidunderlige læsning !!! Jeg kunne bestemt virkelig godt lide hver eneste lille smule af det, og jeg
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
Tak skal du have!|Olá, creio que este é um excelente blogue. Tropecei nele;
že spousta z něj se objevuje na internetu bez mého souhlasu.
Muito obrigado!}
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
Hmm it looks like your blog ate my first comment (it was extremely long) so I guess I’ll just sum it up what I submitted and say, I’m thoroughly enjoying your blog. I too am an aspiring blog writer but I’m still new to the whole thing. Do you have any recommendations for inexperienced blog writers? I’d really appreciate it.
Obrigado|Olá a todos, os conteúdos existentes nesta
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
I’m not sure exactly why but this site is loading extremely slow for me. Is anyone else having this problem or is it a problem on my end? I’ll check back later and see if the problem still exists.
I am curious to find out what blog platform you have been working with? I’m having some small security issues with my latest site and I would like to find something more safeguarded. Do you have any suggestions?
Pretty nice post. I just stumbled upon your weblog and wished to say that I have truly enjoyed browsing your blog posts. After all I will be subscribing to your feed and I hope you write again soon!
Hello there, You have done an incredible job. I will definitely digg it and personally recommend to my friends. I’m confident they will be benefited from this website.
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
gruppe? Der er mange mennesker, som jeg tror virkelig ville
meget af det dukker op overalt på internettet uden min aftale.
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
Hey there would you mind letting me know which hosting company you’re using? I’ve loaded your blog in 3 completely different browsers and I must say this blog loads a lot quicker then most. Can you recommend a good hosting provider at a honest price? Cheers, I appreciate it!
Hi there! Someone in my Facebook group shared this website with us so I came to check it out. I’m definitely loving the information. I’m bookmarking and will be tweeting this to my followers! Terrific blog and superb style and design.
Hi there just wanted to give you a brief heads up and let you know a few of the images aren’t loading correctly. I’m not sure why but I think its a linking issue. I’ve tried it in two different internet browsers and both show the same outcome.
Music began playing any time I opened this internet site, so irritating!
information.|My family members every time say that I am killing my time here
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
The very root of your writing whilst sounding agreeable initially, did not really settle well with me personally after some time. Somewhere throughout the paragraphs you managed to make me a believer unfortunately only for a short while. I still have a problem with your leaps in logic and one might do well to help fill in all those gaps. When you can accomplish that, I will certainly end up being amazed.
har også bogmærket dig for at se på nye ting på din blog Hej! Har du noget imod, hvis jeg deler din blog med min facebook
skupině? Je tu spousta lidí, o kterých si myslím, že by se opravdu
) Jeg vil besøge igen, da jeg har bogmærket det. Penge og frihed er den bedste måde at ændre sig på, må du være rig og
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
Hey! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche. Your blog provided us useful information to work on. You have done a outstanding job!
We stumbled over here from a different web page and thought I might as well check things out. I like what I see so i am just following you. Look forward to going over your web page repeatedly.
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
Também tenho o seu livro marcado para ver coisas novas no seu blog.
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
Obrigado|Olá a todos, os conteúdos existentes nesta
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
ocenili váš obsah. Dejte mi prosím vědět.
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
webside er virkelig bemærkelsesværdig for folks oplevelse, godt,
) Znovu ho navštívím, protože jsem si ho poznamenal. Peníze a svoboda je nejlepší způsob, jak se změnit, ať jste bohatí a
Também tenho o seu livro marcado para ver coisas novas no seu blog.
muito dele está a aparecer em toda a Internet sem o meu acordo.
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
devido a esta maravilhosa leitura!!! O que é que eu acho?
for the reason that here every material is quality based
Fiquei muito feliz em descobrir este site. Preciso de agradecer pelo vosso tempo
devido a esta maravilhosa leitura!!! O que é que eu acho?
e dizer que gosto muito de ler os vossos blogues.
With havin so much content and articles do you ever run into any problems of plagorism or copyright violation? My website has a lot of unique content I’ve either created myself or outsourced but it looks like a lot of it is popping it up all over the internet without my agreement. Do you know any methods to help reduce content from being stolen? I’d definitely appreciate it.
que eu mesmo criei ou terceirizei, mas parece que
enten oprettet mig selv eller outsourcet, men det ser ud til
fortsæt med at guide andre. Jeg var meget glad for at afdække dette websted. Jeg er nødt til at takke dig for din tid
apreciariam o seu conteúdo. Por favor, me avise.
apreciariam o seu conteúdo. Por favor, me avise.
že spousta z něj se objevuje na internetu bez mého souhlasu.
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
enten oprettet mig selv eller outsourcet, men det ser ud til
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
Obrigado|Olá a todos, os conteúdos existentes nesta
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
I was very happy to uncover this web site. I need to to thank you for your time due to this wonderful read!! I definitely really liked every little bit of it and i also have you book-marked to look at new things on your blog.
Muito obrigado!}
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
ocenili váš obsah. Dejte mi prosím vědět.
Thank you, I have been seeking for information about this subject for ages and yours is the best I’ve discovered so far.
Wonderful beat ! I would like to apprentice while you amend your site, how could i subscribe for a blog website? The account helped me a acceptable deal. I had been tiny bit acquainted of this your broadcast offered bright clear idea
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
I do not even know how I ended up here, but I thought this post was great. I don’t know who you are but certainly you’re going to a famous blogger if you are not already 😉 Cheers!
Good day! This is my first visit to your blog! We are a collection of volunteers and starting a new project in a community in the same niche. Your blog provided us valuable information to work on. You have done a extraordinary job!
for the reason that here every material is quality based
I’m really enjoying the design and layout of your website. It’s a very easy on the eyes which makes it much more enjoyable for me to come here and visit more often. Did you hire out a developer to create your theme? Great work!
Admiring the commitment you put into your blog and detailed information you provide. It’s great to come across a blog every once in a while that isn’t the same out of date rehashed information. Excellent read! I’ve saved your site and I’m adding your RSS feeds to my Google account.
It is appropriate time to make some plans for the future and it’s time to be happy. I’ve read this post and if I could I wish to suggest you some interesting things or suggestions. Maybe you could write next articles referring to this article. I wish to read more things about it!
|Tato stránka má rozhodně všechny informace, které jsem o tomto tématu chtěl a nevěděl jsem, koho se zeptat.|Dobrý den! Tohle je můj 1. komentář tady, takže jsem chtěl jen dát rychlý
Kan du anbefale andre blogs / websteder / fora, der beskæftiger sig med de samme emner?
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
Com tanto conteúdo e artigos, alguma vez se deparou com problemas de plágio ou violação de direitos de autor? O meu site tem muito conteúdo exclusivo que eu próprio criei ou
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
det. Denne side har bestemt alle de oplysninger, jeg ønskede om dette emne, og vidste ikke, hvem jeg skulle spørge. Dette er min 1. kommentar her, så jeg ville bare give en hurtig
I was recommended this website by my cousin. I am not sure whether this post is written by him as nobody else know such detailed about my trouble. You are wonderful! Thanks!
har også bogmærket dig for at se på nye ting på din blog Hej! Har du noget imod, hvis jeg deler din blog med min facebook
reading this weblog’s post to be updated daily.
devido a esta maravilhosa leitura!!! O que é que eu acho?
Tak Hej der til alle, det indhold, der findes på denne
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
Conhecem algum método para ajudar a evitar que o conteúdo seja roubado? Agradecia imenso.
enten oprettet mig selv eller outsourcet, men det ser ud til
enten oprettet mig selv eller outsourcet, men det ser ud til
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
e dizer que gosto muito de ler os vossos blogues.
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
Com tanto conteúdo e artigos, alguma vez se deparou com problemas de plágio ou violação de direitos de autor? O meu site tem muito conteúdo exclusivo que eu próprio criei ou
reading this weblog’s post to be updated daily.
Very good blog! Do you have any hints for aspiring writers? I’m hoping to start my own website soon but I’m a little lost on everything. Would you advise starting with a free platform like WordPress or go for a paid option? There are so many options out there that I’m totally confused .. Any suggestions? Thank you!
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
I’m not that much of a internet reader to be honest but your sites really nice, keep it up! I’ll go ahead and bookmark your website to come back down the road. Many thanks
This design is steller! You definitely know how to keep a reader entertained. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job. I really loved what you had to say, and more than that, how you presented it. Too cool!
|Tato stránka má rozhodně všechny informace, které jsem o tomto tématu chtěl a nevěděl jsem, koho se zeptat.|Dobrý den! Tohle je můj 1. komentář tady, takže jsem chtěl jen dát rychlý
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
Obrigado|Olá a todos, os conteúdos existentes nesta
at web, except I know I am getting familiarity all the time by reading thes pleasant posts.|Fantastic post. I will also be handling some of these problems.|Hello, I think this is a great blog. I happened onto it;) I have bookmarked it and will check it out again. The best way to change is via wealth and independence. May you prosper and never stop mentoring others.|I was overjoyed to find this website. I must express my gratitude for your time because this was an amazing read! I thoroughly enjoyed reading it, and I’ve bookmarked your blog so I can check out fresh content in the future.|Hi there! If I shared your blog with my Facebook group, would that be okay? I believe there are a lot of people who would truly value your article.|منشور رائع. سأتعامل مع بعض هذه|
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
I do love the manner in which you have presented this specific situation and it does give me personally some fodder for consideration. Nonetheless, through just what I have seen, I really wish as other commentary pile on that people remain on point and in no way start on a soap box involving some other news of the day. Anyway, thank you for this exceptional point and although I can not agree with the idea in totality, I respect the point of view.
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
Můžete mi doporučit nějaké další blogy / webové stránky / fóra, které se zabývají stejnými tématy?
Também tenho o seu livro marcado para ver coisas novas no seu blog.
Its like you read my mind! You seem to know so much about this, like you wrote the book in it or something. I think that you can do with some pics to drive the message home a little bit, but instead of that, this is fantastic blog. A fantastic read. I’ll definitely be back.
Attractive section of content. I just stumbled upon your weblog and in accession capital to assert that I get in fact enjoyed account your blog posts. Anyway I’ll be subscribing to your feeds and even I achievement you access consistently quickly.
at web, except I know I am getting familiarity all the time by reading thes pleasant posts.|Fantastic post. I will also be handling some of these problems.|Hello, I think this is a great blog. I happened onto it;) I have bookmarked it and will check it out again. The best way to change is via wealth and independence. May you prosper and never stop mentoring others.|I was overjoyed to find this website. I must express my gratitude for your time because this was an amazing read! I thoroughly enjoyed reading it, and I’ve bookmarked your blog so I can check out fresh content in the future.|Hi there! If I shared your blog with my Facebook group, would that be okay? I believe there are a lot of people who would truly value your article.|منشور رائع. سأتعامل مع بعض هذه|
værdsætter dit indhold. Lad mig venligst vide det.
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
værdsætter dit indhold. Lad mig venligst vide det.
This is a terrific web page, will you be involved in doing an interview about how you developed it? If so e-mail me!
Hmm is anyone else experiencing problems with the images on this blog loading? I’m trying to find out if its a problem on my end or if it’s the blog. Any suggestions would be greatly appreciated.
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
nogensinde løbe ind i problemer med plagorisme eller krænkelse af ophavsretten? Mit websted har en masse unikt indhold, jeg har
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
|Tato stránka má rozhodně všechny informace, které jsem o tomto tématu chtěl a nevěděl jsem, koho se zeptat.|Dobrý den! Tohle je můj 1. komentář tady, takže jsem chtěl jen dát rychlý
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
buď vytvořil sám, nebo zadal externí firmě, ale vypadá to.
I’m not that much of a online reader to be honest but your sites really nice, keep it up! I’ll go ahead and bookmark your site to come back down the road. All the best
Hey I am so delighted I found your blog, I really found you by mistake, while I was browsing on Bing for something else, Anyhow I am here now and would just like to say thanks a lot for a fantastic post and a all round interesting blog (I also love the theme/design), I don’t have time to go through it all at the minute but I have book-marked it and also added your RSS feeds, so when I have time I will be back to read a great deal more, Please do keep up the excellent work.
At this time it sounds like BlogEngine is the preferred blogging platform out there right now. (from what I’ve read) Is that what you are using on your blog?
Hey! Would you mind if I share your blog with my zynga group? There’s a lot of people that I think would really appreciate your content. Please let me know. Thank you
díky tomuto nádhernému čtení! Rozhodně se mi líbil každý kousek z toho a já
Tak skal du have!|Olá, creio que este é um excelente blogue. Tropecei nele;
Tak skal du have!|Olá, creio que este é um excelente blogue. Tropecei nele;
) Znovu ho navštívím, protože jsem si ho poznamenal. Peníze a svoboda je nejlepší způsob, jak se změnit, ať jste bohatí a
Tak skal du have!|Olá, creio que este é um excelente blogue. Tropecei nele;
meget af det dukker op overalt på internettet uden min aftale.
apreciariam o seu conteúdo. Por favor, me avise.
devido a esta maravilhosa leitura!!! O que é que eu acho?
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
Conhecem algum método para ajudar a evitar que o conteúdo seja roubado? Agradecia imenso.
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
fortsæt med at guide andre. Jeg var meget glad for at afdække dette websted. Jeg er nødt til at takke dig for din tid
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
at web, except I know I am getting familiarity all the time by reading thes pleasant posts.|Fantastic post. I will also be handling some of these problems.|Hello, I think this is a great blog. I happened onto it;) I have bookmarked it and will check it out again. The best way to change is via wealth and independence. May you prosper and never stop mentoring others.|I was overjoyed to find this website. I must express my gratitude for your time because this was an amazing read! I thoroughly enjoyed reading it, and I’ve bookmarked your blog so I can check out fresh content in the future.|Hi there! If I shared your blog with my Facebook group, would that be okay? I believe there are a lot of people who would truly value your article.|منشور رائع. سأتعامل مع بعض هذه|
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
muito dele está a aparecer em toda a Internet sem o meu acordo.
har også bogmærket dig for at se på nye ting på din blog Hej! Har du noget imod, hvis jeg deler din blog med min facebook
Můžete mi doporučit nějaké další blogy / webové stránky / fóra, které se zabývají stejnými tématy?
) Jeg vil besøge igen, da jeg har bogmærket det. Penge og frihed er den bedste måde at ændre sig på, må du være rig og
enten oprettet mig selv eller outsourcet, men det ser ud til
information.|My family members every time say that I am killing my time here
Kan du anbefale andre blogs / websteder / fora, der beskæftiger sig med de samme emner?
apreciariam o seu conteúdo. Por favor, me avise.
Com tanto conteúdo e artigos, alguma vez se deparou com problemas de plágio ou violação de direitos de autor? O meu site tem muito conteúdo exclusivo que eu próprio criei ou
Conhecem algum método para ajudar a evitar que o conteúdo seja roubado? Agradecia imenso.
reading this weblog’s post to be updated daily.
værdsætter dit indhold. Lad mig venligst vide det.
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
Můžete mi doporučit nějaké další blogy / webové stránky / fóra, které se zabývají stejnými tématy?
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
e dizer que gosto muito de ler os vossos blogues.
enten oprettet mig selv eller outsourcet, men det ser ud til
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
|Tato stránka má rozhodně všechny informace, které jsem o tomto tématu chtěl a nevěděl jsem, koho se zeptat.|Dobrý den! Tohle je můj 1. komentář tady, takže jsem chtěl jen dát rychlý
que eu mesmo criei ou terceirizei, mas parece que
Podem recomendar outros blogues/sites/fóruns que tratem dos mesmos temas?
nogensinde løbe ind i problemer med plagorisme eller krænkelse af ophavsretten? Mit websted har en masse unikt indhold, jeg har
e dizer que gosto muito de ler os vossos blogues.
meget af det dukker op overalt på internettet uden min aftale.
) Znovu ho navštívím, protože jsem si ho poznamenal. Peníze a svoboda je nejlepší způsob, jak se změnit, ať jste bohatí a
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
Obrigado|Olá a todos, os conteúdos existentes nesta
Tak skal du have!|Olá, creio que este é um excelente blogue. Tropecei nele;
nenarazili jste někdy na problémy s plagorismem nebo porušováním autorských práv? Moje webové stránky mají spoustu unikátního obsahu, který jsem vytvořil.
muito dele está a aparecer em toda a Internet sem o meu acordo.
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
Muito obrigado!}
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
skupině? Je tu spousta lidí, o kterých si myslím, že by se opravdu
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
I will revisit once again since i have book-marked it. Money and freedom is the best way to change, may you be rich and continue to guide others.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
buď vytvořil sám, nebo zadal externí firmě, ale vypadá to.
ocenili váš obsah. Dejte mi prosím vědět.
ocenili váš obsah. Dejte mi prosím vědět.
Tak Hej der til alle, det indhold, der findes på denne
Muito obrigado!}
Our skillset in cyber finance and online transactions means we’re perfectly equipped to tackle your QIWI wallet issues.Have peace of mind, we utilize state-of-the-art techniques and stayupdated with the latest fraud prevention strategies.In case of affected by unauthorized transactions or technical glitches that caused a loss of funds, we’rehere to help.
学生証・滞在許可証をご提出頂きます。1957年のイギリスからの独立以来、一貫して政権を維持している保守政権の下、国内総生産(GDP)はアジア諸国連合(ASEAN)の中でも2位となっており、現在も成長し続けている国となっています。特に、総合商社の華やかなイメージの裏側にある、いわば泥臭い舞台裏にスポットを当てました。応募総数916名(229チーム)の中から選考を突破したチームが、それぞれ東京では13、大阪では11チーム参加しました。 また、WIN以外の提携プログラムや個人で応募・
College of Alabama Press.
Needed to send you that very little word just to thank you very much again for these striking strategies you have documented above. It was really incredibly generous of people like you to allow publicly all that a lot of people would have offered for sale as an ebook to make some bucks for their own end, specifically seeing that you could possibly have done it if you considered necessary. Those basics as well acted as the easy way to realize that some people have a similar interest just as my personal own to understand good deal more around this condition. I’m certain there are millions of more pleasurable situations up front for those who looked at your website.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
I’m still learning from you, but I’m trying to achieve my goals. I certainly liked reading all that is written on your site.Keep the stories coming. I liked it!
вывод из запоя на дому ростов ekonomimvmeste.ukrbb.net/viewtopic.php?f=14&t=65331 .
Nikmati permainan slot online terbaik di Kantorbola, bandar slot terpercaya 2025. Raih jackpot besar dan hadiah melimpah setiap hari. Daftar sekarang untuk bonus eksklusif.
Hi there, I do believe your web site could be having browser compatibility problems. Whenever I look at your site in Safari, it looks fine however when opening in Internet Explorer, it’s got some overlapping issues. I simply wanted to provide you with a quick heads up! Aside from that, great blog.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Regards! An abundance of forum posts!
لماذا YYY هو الخيار الأول للاعبين العربلماذا YYY هو الخيار الأول للاعبين العربيتم تحسين كازينو YYY بدقة لتفضيلات اللاعبين العرب.لا تقتصر منصتنا على واجهة باللغة العربية فحسب،بل تشمل أيضًا تكيفات إقليمية ت resonates بعمق مع لاعبينا.فريق دعم العملاء لدينا، الذي يتقن اللغة العربية، متواجد على مدار الساعة طوال أيامالأسبوع لمساعدتك في أي استفسارات أو للاحتفال بانتصاراتك معك.مع فهم القلب الثقافي للألعاب في العالمالعربي، نحن نكرم هذه التقاليدمع لمسة عصرية. تتراوح عروضنا من ألعاب الطاولة الكلاسيكية التي يعتز بها الأجيال في المنطقة إلى الفتحات المبتكرة التي تجلب الإثارة الجديدة.في كازينو YYY، ترقص التقاليد والحداثة في انسجام، مما يوفر تجربة لعب تجمع بينالألفة والإثارة.كازينو YYY ليس مجرد منصة؛ إنه عالم من الأناقة.كل عنصر، من واجهة المستخدم إلى رسومات اللعبة، مصمم للراحة والرضا وتجربةبصرية مذهلة. التنقل سهل، مما يتيح لك الانتقال بسلاسة من لعبة إلى أخرى، والانغماس في عالم المقامرة عبر الإنترنت بأناقة وسهولة.ترقبوا المزيد حول ما يجعل كازينو YYY الوجهة النهائية للاعبين العرب.من المكافآت السخية وتنوع الألعاب إلى الميزاتالفريدة التي تميزنا، اكتشفلماذا يعتبر كازينو YYY أفضل كازينو عربي على الإنترنت.مكافآت كازينو YYY
Your article helped me a lot, is there any more related content? Thanks!
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
Thank you for your shening. I am worried that I lack creative ideas. It is your enticle that makes me full of hope. Thank you. But, I have a question, can you help me?
Your article helped me a lot, is there any more related content? Thanks!
e dizer que gosto muito de ler os vossos blogues.
Some truly interesting information, well written and loosely user genial.
Ray Esports – Lựa chọn hàng đầu cho người yêu thích cá cược thể thao điện tử, nơi bạn có thể tham gia kèo cược đa dạng với tỷ lệ hấp dẫn và hệ thống bảo mật cao.
Với hệ thống bảo mật nhiều lớp, Ray Esports cam kết bảo vệ thông tin người chơi, đảm bảo giao dịch an toàn, nhanh chóng và trải nghiệm cá cược công bằng, minh bạch.
Ray Esports – Hệ thống cá cược esports chuẩn quốc tế, tích hợp công nghệ mã hóa dữ liệu, bảo vệ thông tin người chơi và cam kết rút tiền nhanh, thanh toán chính xác.
Đặt cược esports dễ dàng và an toàn tại Ray Esports, nền tảng cá cược chuyên nghiệp với hệ thống bảo mật tiên tiến, đảm bảo mọi giao dịch đều nhanh chóng và minh bạch.
Tham gia Ray Esports để trải nghiệm cá cược esports đẳng cấp với hệ thống giao dịch nhanh chóng, minh bạch và hỗ trợ người chơi 24/7, đảm bảo công bằng và thuận tiện.
Ray Esports mang đến nền tảng cá cược esports chuyên nghiệp, đảm bảo tính minh bạch, bảo mật cao, hỗ trợ người chơi 24/7 và cung cấp hàng loạt kèo cược hấp dẫn trên nhiều tựa game hot.
Ray Esports – Hệ thống cá cược thể thao điện tử đáng tin cậy, cung cấp tỷ lệ cược chính xác, giao dịch nhanh chóng và an toàn, hỗ trợ đa dạng tựa game từ LMHT, CS:GO, Dota 2 đến Valorant.
Đồng hành cùng Ray Esports, tận hưởng nền tảng cá cược esports hiện đại với tỷ lệ cược hấp dẫn cho các tựa game đình đám như League of Legends, CS:GO, Dota 2, Valorant, FIFA Online…
Můžete mi doporučit nějaké další blogy / webové stránky / fóra, které se zabývají stejnými tématy?
I think the admin of this web site is actually working hardin support of his web page, as here every stuff is quality basedinformation.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
Magnificent site. A lot of helpful information here. I’m sending it to a few friends ans additionally sharing in delicious. And of course, thank you to your effort!
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
1m7VNdW9
I was more than happy to find this site. I want to to thank you for ones time due to this wonderful read!! I definitely savored every part of it and I have you book-marked to look at new things on your blog.
Greetings, I do think your web site might be having internet browser compatibility issues. When I take a look at your web site in Safari, it looks fine but when opening in I.E., it has some overlapping issues. I simply wanted to provide you with a quick heads up! Besides that, fantastic website!
It’s difficult to find experienced people for this subject, but you sound like you know what you’re talking about! Thanks
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Hi! Do you know if they make any plugins to protect against hackers? I’m kinda paranoid about losing everything I’ve worked hard on. Any tips?
Đồng hành cùng Ray Esports, tận hưởng nền tảng cá cược esports hiện đại với tỷ lệ cược hấp dẫn cho các tựa game đình đám như League of Legends, CS:GO, Dota 2, Valorant, FIFA Online…
Ray Esports – Nền tảng cá cược esports hàng đầu, hỗ trợ giao dịch nhanh chóng, bảo mật an toàn tuyệt đối, cùng hàng loạt ưu đãi hấp dẫn dành riêng cho game thủ đam mê thể thao điện tử.
Ray Esports – Lựa chọn hàng đầu cho người yêu thích cá cược thể thao điện tử, nơi bạn có thể tham gia kèo cược đa dạng với tỷ lệ hấp dẫn và hệ thống bảo mật cao.
Ray Esports – Sự lựa chọn đáng tin cậy cho cộng đồng cá cược esports, mang đến trải nghiệm mượt mà, giao dịch nhanh, dịch vụ tận tâm và môi trường công bằng.
Tham gia Ray Esports, tận hưởng nền tảng cá cược esports chuẩn quốc tế, cam kết bảo mật thông tin người chơi, xử lý giao dịch nhanh, rút tiền an toàn và hỗ trợ 24/7.
Ray Esports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game hot như LMHT, Dota 2, CS:GO, Valorant, PUBG…
No matter if some one searches for his vital thing, thushe/she desires to be available that in detail, therefore that thing ismaintained over here.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Great write-up, I am normal visitor of one?¦s website, maintain up the excellent operate, and It is going to be a regular visitor for a long time.
集合住宅不動産を手掛ける同社は稼働前の22年8月、ベンチャーキャピタル(VC)のアンドリーセン・自身のYouTube配信内で、日本人には「ビビリ」が多いとし、その理由について、アフリカ人には「恐怖」のDNAを持っていない人が多く、やりたいことがあれば「ビビる」ことなくやるが、アジア人はアフリカで負けてヨーロッパに渡り、ヨーロッパで負けて中東に行き、中東で負けて東南アジアに行き、東南アジアで負けて日本に来たが日本で逃げる先がなく、そこで凍えて暮らしていたのが日本人のルーツであるため、日本人は基本「ビビリ」の集合体であると主張した。
Peach, Wash. October 7, 1930.
Với nhiều năm kinh nghiệm trong lĩnh vực cá cược esports, Ray Esports mang đến nền tảng hiện đại, giao dịch nhanh chóng, hệ thống bảo mật cao và dịch vụ hỗ trợ tận tình.
Cam kết an toàn, minh bạch, Ray Esports hợp tác với các giải đấu esports hàng đầu, đảm bảo hệ thống cá cược công bằng, giao dịch nhanh và chính xác cho mọi người chơi.
Tham gia Ray Esports để trải nghiệm cá cược esports đẳng cấp với hệ thống giao dịch nhanh chóng, minh bạch và hỗ trợ người chơi 24/7, đảm bảo công bằng và thuận tiện.
Ray Esports – Hệ thống cá cược esports chuẩn quốc tế, tích hợp công nghệ mã hóa dữ liệu, bảo vệ thông tin người chơi và cam kết rút tiền nhanh, thanh toán chính xác.
Với hệ thống bảo mật nhiều lớp, Ray Esports cam kết bảo vệ thông tin người chơi, đảm bảo giao dịch an toàn, nhanh chóng và trải nghiệm cá cược công bằng, minh bạch.
Trải nghiệm cá cược esports đỉnh cao tại Ray Esports – nơi bạn có thể đặt cược trực tiếp vào các giải đấu lớn của LMHT, Dota 2, CS:GO, Valorant, PUBG Mobile và nhiều tựa game khác.
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2…
Cam kết minh bạch và an toàn, Rbviet.net Rbesports hợp tác cùng các giải đấu esports lớn, đảm bảo hệ thống cá cược công bằng và giao dịch chính xác, nhanh chóng.
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám.
Tham gia Rbviet.net Rbesports để trải nghiệm cá cược esports chuẩn quốc tế, bảo mật thông tin tuyệt đối, rút tiền nhanh chóng và dịch vụ hỗ trợ liên tục 24/7.
Với kinh nghiệm dày dặn trong cá cược esports, Rbviet.net Rbesports mang đến nền tảng hiện đại, giao dịch siêu tốc, bảo mật tuyệt đối và dịch vụ hỗ trợ tận tâm.
Rbviet.net Rbesports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game đỉnh cao như LMHT, Dota 2, CS:GO, Valorant, PUBG…
Rbviet.net Rbesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến.
Tham gia ngay Rbviet.net Rbesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn.
Rbviet.net Rbesports mang đến hệ thống cá cược esports chuyên nghiệp, đảm bảo tính minh bạch, bảo mật cao cấp, hỗ trợ 24/7 và kèo cược hấp dẫn trên mọi tựa game hot. – 2025 March 17, 17:17
Tham gia Rbviet.net Rbesports để trải nghiệm cá cược esports đẳng cấp, giao dịch minh bạch, hỗ trợ 24/7 và cam kết mang đến sự công bằng, tiện lợi cho người chơi. – 2025 March 17, 17:19
Rbviet.net Rbesports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game đỉnh cao như LMHT, Dota 2, CS:GO, Valorant, PUBG… – 2025 March 17, 17:21
Rbviet.net Rbesports – Điểm đến đáng tin cậy của cộng đồng cá cược esports, mang lại trải nghiệm mượt mà, giao dịch nhanh và dịch vụ chăm sóc khách hàng chu đáo. – 2025 March 17, 17:23
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 17, 17:24
Tham gia ngay Rbviet.net Rbesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn. – 2025 March 18, 11:38
Cam kết minh bạch và an toàn, Rbviet.net Rbesports hợp tác cùng các giải đấu esports lớn, đảm bảo hệ thống cá cược công bằng và giao dịch chính xác, nhanh chóng. – 2025 March 18, 11:45
Đặt cược esports an toàn, dễ dàng tại Rbviet.net Rbesports, nền tảng chuyên nghiệp với công nghệ bảo mật hiện đại, đảm bảo giao dịch nhanh chóng và minh bạch. – 2025 March 18, 11:47
Cam kết minh bạch và an toàn, Rbviet.net Rbesports hợp tác cùng các giải đấu esports lớn, đảm bảo hệ thống cá cược công bằng và giao dịch chính xác, nhanh chóng. – 2025 March 18, 11:50
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 18, 11:52
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 March 18, 11:56
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 18, 11:58
Tham gia ngay Rbviet.net Rbesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn. – 2025 March 18, 13:39
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 18, 13:42
Đặt cược esports an toàn, dễ dàng tại Rbviet.net Rbesports, nền tảng chuyên nghiệp với công nghệ bảo mật hiện đại, đảm bảo giao dịch nhanh chóng và minh bạch. – 2025 March 18, 13:44
Rbviet.net Rbesports – Điểm đến đáng tin cậy của cộng đồng cá cược esports, mang lại trải nghiệm mượt mà, giao dịch nhanh và dịch vụ chăm sóc khách hàng chu đáo. – 2025 March 18, 13:46
Rbviet.net Rbesports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game đỉnh cao như LMHT, Dota 2, CS:GO, Valorant, PUBG… – 2025 March 18, 13:48
Khám phá Rbviet.net Rbesports – Nền tảng cá cược esports hiện đại, cung cấp tỷ lệ cược hấp dẫn, giao dịch an toàn và dịch vụ hỗ trợ chuyên nghiệp cho game thủ. – 2025 March 18, 13:54
Rbviet.net Rbesports đồng hành cùng các sự kiện esports tầm cỡ, cung cấp môi trường cá cược chuyên nghiệp với giao dịch nhanh chóng, bảo mật tối ưu và hỗ trợ liên tục 24/7. – 2025 March 18, 13:57
Rbviet.net Rbesports mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 March 18, 13:59
Rbviet.net Rbesports mang đến hệ thống cá cược esports chuyên nghiệp, đảm bảo tính minh bạch, bảo mật cao cấp, hỗ trợ 24/7 và kèo cược hấp dẫn trên mọi tựa game hot. – 2025 March 19, 12:32
Tham gia Rbviet.net Rbesports để trải nghiệm cá cược esports chuẩn quốc tế, bảo mật thông tin tuyệt đối, rút tiền nhanh chóng và dịch vụ hỗ trợ liên tục 24/7. – 2025 March 19, 12:34
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 19, 12:37
Rbviet.net Rbesports mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 March 19, 12:39
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 March 19, 12:42
Tham gia ngay Rbviet.net Rbesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn. – 2025 March 19, 12:47
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 19, 12:50
Với kinh nghiệm dày dặn trong cá cược esports, Rbviet.net Rbesports mang đến nền tảng hiện đại, giao dịch siêu tốc, bảo mật tuyệt đối và dịch vụ hỗ trợ tận tâm. – 2025 March 19, 12:52
information.|My family members every time say that I am killing my time here
I visited a lot of website but I conceive this one contains something special in it.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Choose BWER for trusted weighbridge systems in Iraq, offering customized solutions to optimize your industrial operations and ensure precise weight measurement every time.
These are actually fantastic ideas in regardingblogging. You have touched some nice things here.Any way keep up wrinting.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
Oh my goodness! Awesome article dude! Thank you, However I am encountering problems with your RSS. I don’t understand why I am unable to join it. Is there anybody else having identical RSS issues? Anyone who knows the solution will you kindly respond? Thanks.
Rbviet.net Rbesports mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 March 21, 09:11
Rbviet.net Rbesports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game đỉnh cao như LMHT, Dota 2, CS:GO, Valorant, PUBG… – 2025 March 21, 09:13
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 21, 09:15
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 21, 09:17
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 March 21, 09:20
Rbviet.net Rbesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 March 21, 09:25
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 21, 09:27
Rbviet.net Rbesports – Nền tảng cá cược esports hàng đầu với giao dịch siêu tốc, bảo mật an toàn tuyệt đối và nhiều ưu đãi độc quyền dành cho fan thể thao điện tử. – 2025 March 21, 09:29
Hi, this weekend is fastidious designed for me, since this point in time i am reading this impressiveinformative piece of writing here at my residence.
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
Nicely put, Thanks a lot.
They took us by bus to the airport.
Sadly, they share a division with two of baseball’s hardest groups, the Yankees and Red Sox so bringing a World Collection to Oriole Park at Camden Yards will probably be quite the problem.
形勢が相当に不利であっても投了せずに指しつづける。展示ブースの内容は出展社の担当者が簡単に書き替える事ができるので常に最新情報に更新されています。出展にかかる費用の大きな内訳として、出展料とブースのコンテンツ制作料があります。 これは.jp第14話でロディのパチモンを出したところ、版元のJAMMYから「どうせ出すなら本物出して」という要請があったため実現した。現実世界では警察署の落し物の窓口係をしており、サイバー空間に来られるのは休憩時間のみ。物理的な世界とデジタルの世界を融合させるハードウェアとソフトウェアのソリューションによって、次世代のユーザーインタラクションの到来を提供しています。 インターナショナル日本支部」の創設メンバーの川田泰代が名前を連ねるなど、執筆の世界とも所縁が深い。
Professor Emeritus of Bacteriology, University of London.
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 March 24, 16:06
Rbviet.net Rbesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 March 24, 16:08
Cam kết minh bạch và an toàn, Rbviet.net Rbesports hợp tác cùng các giải đấu esports lớn, đảm bảo hệ thống cá cược công bằng và giao dịch chính xác, nhanh chóng. – 2025 March 24, 16:11
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 24, 16:13
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 24, 16:15
Rbviet.net Rbesports mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 March 24, 16:20
Rbviet.net Rbesports mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 March 24, 16:23
Rbviet.net Rbesports mang đến hệ thống cá cược esports chuyên nghiệp, đảm bảo tính minh bạch, bảo mật cao cấp, hỗ trợ 24/7 và kèo cược hấp dẫn trên mọi tựa game hot. – 2025 March 24, 16:25
Rbviet.net Rbesports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game đỉnh cao như LMHT, Dota 2, CS:GO, Valorant, PUBG… – 2025 March 25, 11:17
Tham gia Rbviet.net Rbesports để trải nghiệm cá cược esports đẳng cấp, giao dịch minh bạch, hỗ trợ 24/7 và cam kết mang đến sự công bằng, tiện lợi cho người chơi. – 2025 March 25, 11:19
Với công nghệ bảo mật đa tầng, Rbviet.net Rbesports cam kết bảo vệ thông tin người chơi, giao dịch an toàn, nhanh gọn và mang đến trải nghiệm cá cược công bằng. – 2025 March 25, 11:21
Rbviet.net Rbesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 March 25, 11:23
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 25, 11:25
Rbviet.net Rbesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 March 25, 11:29
Tham gia ngay Rbviet.net Rbesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn. – 2025 March 25, 11:31
Rbviet.net Rbesports – Nền tảng cá cược esports hàng đầu với giao dịch siêu tốc, bảo mật an toàn tuyệt đối và nhiều ưu đãi độc quyền dành cho fan thể thao điện tử. – 2025 March 25, 11:33
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 25, 14:24
Rbviet.net Rbesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 March 25, 14:26
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 March 25, 14:31
Với kinh nghiệm dày dặn trong cá cược esports, Rbviet.net Rbesports mang đến nền tảng hiện đại, giao dịch siêu tốc, bảo mật tuyệt đối và dịch vụ hỗ trợ tận tâm. – 2025 March 25, 14:34
Trải nghiệm cá cược esports đỉnh cao tại Rbviet.net Rbesports – nơi bạn có thể tham gia đặt cược trực tiếp vào các giải đấu lớn của LMHT, Dota 2, CS:GO, Valorant và nhiều tựa game khác. – 2025 March 25, 14:39
Khám phá Rbviet.net Rbesports – Nền tảng cá cược esports hiện đại, cung cấp tỷ lệ cược hấp dẫn, giao dịch an toàn và dịch vụ hỗ trợ chuyên nghiệp cho game thủ. – 2025 March 25, 14:41
Rbviet.net Rbesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 March 25, 14:45
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
You are so interesting! I do not suppose I’ve read a single thing like this before. So nice to find another person with a few unique thoughts on this topic. Seriously.. thank you for starting this up. This web site is one thing that’s needed on the web, someone with a bit of originality.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
BMW survived World Conflict II to produce the 507 model, which was not launched till the 1950s.
This excellent website certainly has all the info I wanted about this subject and didn’t know who to ask.
789bet là Sân chơi công bằng, minh bạch, nhân văn kể trên giúp chúng ta cược thể thao, game bài đổi thưởng, bắn cá, slot, lô đề online, đá gà như ý. tại 789bett.asia
Conhecem algum método para ajudar a evitar que o conteúdo seja roubado? Agradecia imenso.
Rbviet.net Rbesports – Hệ thống cá cược esports quốc tế với công nghệ mã hóa tiên tiến, bảo vệ dữ liệu người chơi và đảm bảo thanh toán chính xác, nhanh gọn. – 2025 March 26, 10:08
Rbviet.net Rbesports mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 March 26, 10:10
Rbviet.net Rbesports mang đến hệ thống cá cược esports chuyên nghiệp, đảm bảo tính minh bạch, bảo mật cao cấp, hỗ trợ 24/7 và kèo cược hấp dẫn trên mọi tựa game hot. – 2025 March 26, 10:13
Rbviet.net Rbesports đồng hành cùng các sự kiện esports tầm cỡ, cung cấp môi trường cá cược chuyên nghiệp với giao dịch nhanh chóng, bảo mật tối ưu và hỗ trợ liên tục 24/7. – 2025 March 26, 10:16
Rbviet.net Rbesports – Hệ thống cá cược esports quốc tế với công nghệ mã hóa tiên tiến, bảo vệ dữ liệu người chơi và đảm bảo thanh toán chính xác, nhanh gọn. – 2025 March 26, 10:21
Rbviet.net Rbesports là nền tảng cá cược thể thao điện tử hàng đầu, mang đến trải nghiệm đặt cược trực tiếp cho hơn 10 tựa game đỉnh cao như LMHT, Dota 2, CS:GO, Valorant, PUBG… – 2025 March 26, 10:23
Rbviet.net Rbesports – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 March 26, 10:25
Dapatkan pengalaman trading terbaik dengan belajar di Prof FX! Kami menawarkan bonus forex menarik untuk meningkatkan modal dagangan anda, panduan belajar trading untuk pemula dan profesional, serta kontes forex dengan hadiah lumayan. Temui broker forex terpercaya yang sesuai dengan gaya dagangan anda dan mulakan perjalanan trading anda hari ini!
If some one needs expert view rsgarding running a blog then i recommend him/her to pay a quichk visit
this weblog, Keep up the pleasant job. https://Menbehealth.Wordpress.com/
The Billionaire Brain Wave is a digital program designed to help individuals unlock their financial potential by leveraging cutting-edge brainwave technology.
I just added this feed to my bookmarks. I have to say, I really enjoy reading your blogs. Thanks!
Reclaiming what’s yours shouldn’t be troublesome.That’s why our methodology is straightforwardand open.You just need to supply your transaction details, and we’ll manage the rest.Don’t let technical problems prevent you from your hard-earned money.Our goal is to assist you in reclaiming every cent.
Greetings, I do believe your blog could possibly be having browser compatibility issues. Whenever I look at your website in Safari, it looks fine however, when opening in IE, it’s got some overlapping issues. I just wanted to give you a quick heads up! Aside from that, fantastic blog!
It included sixteen colour plates and more than 24 halftone illustrations.
I was curious if you ever thought of changing the layout of your site? Its very well written; I love what youve got to say. But maybe you could a little more in the way of content so people could connect with it better. Youve got an awful lot of text for only having 1 or 2 pictures. Maybe you could space it out better?
Thanks for sharing your info. I really appreciate your efforts andI am waiting for your next write ups thanks once again.
May I just say what a relief to uncover someone that really knows what they’re talking about online. You certainly realize how to bring an issue to light and make it important. A lot more people really need to read this and understand this side of the story. I was surprised that you are not more popular given that you certainly have the gift.
You’ve made some decent points there. I looked on the internet to find out more about the issue and found most individuals will go along with your views on this website.
Enjoyed every bit of your article post. Cool.
Pretty! This was a really wonderful article. Thanks for supplying this info.
f27wyo
Rayesports.com Rayesports – Điểm đến đáng tin cậy của cộng đồng cá cược esports, mang lại trải nghiệm mượt mà, giao dịch nhanh và dịch vụ chăm sóc khách hàng chu đáo. – 2025 April 01, 09:17
Tham gia ngay Rayesports.com Rayesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn. – 2025 April 01, 09:20
Khám phá Rayesports.com Rayesports – Nền tảng cá cược esports hiện đại, cung cấp tỷ lệ cược hấp dẫn, giao dịch an toàn và dịch vụ hỗ trợ chuyên nghiệp cho game thủ. – 2025 April 01, 09:22
Tham gia Rayesports.com Rayesports để trải nghiệm cá cược esports đẳng cấp, giao dịch minh bạch, hỗ trợ 24/7 và cam kết mang đến sự công bằng, tiện lợi cho người chơi. – 2025 April 01, 09:24
Rayesports.com Rayesports – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 April 01, 09:29
Tham gia ngay Rayesports.com Rayesports để tận hưởng cá cược esports chuyên nghiệp, với hệ thống bảo mật hàng đầu, giao dịch siêu tốc và hàng loạt ưu đãi dành riêng cho bạn. – 2025 April 01, 09:32
Rayesports.com Rayesports – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 April 01, 09:35
Rbviet.net Rbviet mang đến trải nghiệm cá cược esports hoàn hảo với kèo cược đa dạng, giao dịch tức thì, bảo mật tối ưu và hỗ trợ mọi lúc mọi nơi. – 2025 April 09, 10:11
Rbviet.net Rbviet – Điểm đến lý tưởng cho cá cược thể thao điện tử, đảm bảo bảo mật cao, giao dịch nhanh và trải nghiệm đặt cược mượt mà trên mọi tựa game đình đám. – 2025 April 09, 10:15
Với kinh nghiệm dày dặn trong cá cược esports, Rbviet.net Rbviet mang đến nền tảng hiện đại, giao dịch siêu tốc, bảo mật tuyệt đối và dịch vụ hỗ trợ tận tâm. – 2025 April 09, 10:17
Rbviet.net Rbviet – Địa chỉ cá cược thể thao điện tử uy tín, cung cấp tỷ lệ cược chính xác, giao dịch an toàn, nhanh chóng và hỗ trợ đa dạng game như LMHT, CS:GO, Dota 2… – 2025 April 09, 10:22
Rbviet.net Rbviet – Lựa chọn số một cho người đam mê cá cược esports, nơi bạn tận hưởng kèo cược đa dạng, tỷ lệ hấp dẫn và hệ thống bảo mật tiên tiến. – 2025 April 09, 10:27
Rbviet.net Rbviet – Điểm đến đáng tin cậy của cộng đồng cá cược esports, mang lại trải nghiệm mượt mà, giao dịch nhanh và dịch vụ chăm sóc khách hàng chu đáo. – 2025 April 09, 10:31
Khám phá Rbviet.net Rbviet – Nền tảng cá cược esports hiện đại, cung cấp tỷ lệ cược hấp dẫn, giao dịch an toàn và dịch vụ hỗ trợ chuyên nghiệp cho game thủ. – 2025 April 09, 10:33
Também tenho o seu livro marcado para ver coisas novas no seu blog.
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
Wildio là một cái tên không còn xa lạ trong giới cá cược trực tuyến tại Việt Nam. Được biết đến là một nền tảng giải trí hấp dẫn, Wildio không chỉ mang đến những trải nghiệm cá cược đỉnh cao mà còn đảm bảo môi trường chơi an toàn và minh bạch. Với sự phát triển nhanh chóng của công nghệ và nhu cầu ngày càng cao của người chơi, Wildio đã khẳng định được vị thế của mình trên thị trường.
Wow, awesome weblog format! How lengthy have you ever been running a blog for? you make running a blog look easy. The total look of your web site is excellent, let alone the content material!
Discover the power of MinSwap, the leading decentralized exchange platform offering seamless trading and low fees. Maximize your assets and join the next generation of decentralized finance
Hello very nice website!! Man .. Beautiful .. Wonderful .. I will bookmark your blog and take the feeds additionally?KI’m satisfied to search out a lot of helpful information right here in the put up, we want develop extra strategies in this regard, thank you for sharing. . . . . .
Your words have resonated with us and we can’t wait to read more of your amazing content. Thank you for sharing your expertise and passion with the world.
翌年2月、卒業後は地元の食品会社への就職が決まった暢子は、高校最後の春休みは東京に行きたいと望む。仙太と言つて、三年の生徒で、新平民の少年がある。 『南太平洋』等の名作ミュージカルで主演するほか、ディナーショー・作中終盤で自身にぶつかってきた末永率いる開久の不良軍団を難なく倒している。
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
стоимость капельницы от запоя стоимость капельницы от запоя .
Hello there! Quick question that’s totally off topic.Do you know how to make your site mobile friendly?My web site looks weird when browsing from my iphone4. I’m trying to find a theme or plugin that mightbe able to correct this issue. If you have anyrecommendations, please share. Cheers!
My brother suggested I might like this blog He was totally right This post actually made my day You can not imagine simply how much time I had spent for this info Thanks
I quite like reading a post that can make people think. Also, thank you for allowing for me to comment.
Com tanto conteúdo e artigos, alguma vez se deparou com problemas de plágio ou violação de direitos de autor? O meu site tem muito conteúdo exclusivo que eu próprio criei ou
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
Bonos de casino Jugabet Per? Bonos de casino Jugabet Per? .
Hi there would you mind sharing which blog platform you’re using? I’m planning to start my own blog soon but I’m having a hard time deciding between BlogEngine/Wordpress/B2evolution and Drupal. The reason I ask is because your layout seems different then most blogs and I’m looking for something completely unique. P.S My apologies for being off-topic but I had to ask!
hey there and thank you for your info – I’ve definitely picked up anything new from right here. I did however expertise several technical points using this website, as I experienced to reload the web site a lot of times previous to I could get it to load correctly. I had been wondering if your web host is OK? Not that I am complaining, but slow loading instances times will very frequently affect your placement in google and could damage your quality score if ads and marketing with Adwords. Anyway I’m adding this RSS to my email and could look out for a lot more of your respective intriguing content. Ensure that you update this again very soon..
Audio began playing when I opened this web site, so irritating!
The root of your writing while sounding agreeable originally, did not really sit very well with me after some time. Someplace throughout the paragraphs you managed to make me a believer but just for a while. I nevertheless have got a problem with your leaps in logic and one might do nicely to help fill in all those breaks. If you actually can accomplish that, I could undoubtedly be amazed.
fantastic points altogether, you just gained a logo new reader. What may you recommend about your post that you made some days in the past? Any certain?
I think this web site has got some rattling good info for everyone :D. “Nothing great was ever achieved without enthusiasm.” by Ralph Waldo Emerson.
I always emailed this web site post page to all my contacts, for the reason that iflike to read it afterward my friends will too.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
WP Lipsum is yet another dummy data generator WordPress plugin, it allows you to add dummy text using Shortcodes and Template tags.
Remarkable! Its genuinely awesome article, I have got much clearidea concerning from this piece of writing.
devido a esta maravilhosa leitura!!! O que é que eu acho?
If you happen to spend money on stock, the worst thing that can happen is that the stock loses completely all of its worth.
After going over a number of the articles on your web page, I honestly appreciate your way of writing a blog. I saved it to my bookmark webpage list and will be checking back soon. Take a look at my website as well and let me know your opinion.
I want to show appreciation to you just for rescuing me from this particular scenario. Just after searching through the world-wide-web and getting methods which were not beneficial, I assumed my entire life was gone. Existing devoid of the answers to the difficulties you have solved by means of your main blog post is a crucial case, as well as the kind which may have adversely affected my career if I hadn’t come across your web site. Your main training and kindness in handling a lot of things was excellent. I don’t know what I would have done if I hadn’t come across such a subject like this. I can at this time look ahead to my future. Thanks a lot so much for this professional and amazing guide. I will not think twice to recommend your web blog to anybody who needs recommendations about this matter.
大栄(以上北栄町)、赤碕(琴浦町)、三朝(三朝町)、大山(大山町)、溝口(伯耆町)、会見・ “山陰合銀、兵庫で法人融資を拡大 企業仲介や海外進出支援”.「合銀、人材紹介会社に出資 副業・ “ごうぎん証券が開業 鳥取、島根に4支店”.
「愛する我子よ。見合いが破綻した直後、章子に罵倒され去られるが、そのまま片島の元にいた章子を連れ戻そうとして口論の末、階段から転落死。 あの背後(うしろ)にしゃがんでいる道化役を御覧。乃木坂46LLC.2022年6月4日閲覧。 Real Sound. blueprint. 2021年6月16日.2021年6月16日閲覧。発売日:1999年6月26日 サンリオ Win/MacハイブリッドCD-ROM仕様。毎日新聞社、1966年/角川文庫(上・祐子のおじゃましまーす– 全日本そっくり大賞 – 欽也のそっくりベスト10 – なるほど!
The Ice Water Hack has gained popularity as a simple yet effective method for boosting metabolism and promoting weight loss.
Our vacation spot marriage ceremony planning companies embody all major points of a wedding including wedding day administration, styling and decoration, full planning service, and partial planning.
Também tenho o seu livro marcado para ver coisas novas no seu blog.
Heya i’m for the first time here. I came across this board and I find It reallyuseful & it helped me out a lot. I hope to give something backand aid others like you aided me.
карниз для штор с электроприводом карниз для штор с электроприводом .
After I originally left a comment I appear to have clicked on the -Notify me when new comments are added- checkbox and now every time a comment is added I get 4 emails with the same comment. Is there a means you are able to remove me from that service? Many thanks.
e dizer que gosto muito de ler os vossos blogues.
webside er virkelig bemærkelsesværdig for folks oplevelse, godt,
Wonderful blog! I found it while searching on Yahoo News. Do you have any tips on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Many thanks
Please let me know if you’re looking for a article writer for your weblog. You have some really good articles and I believe I would be a good asset. If you ever want to take some of the load off, I’d really like to write some content for your blog in exchange for a link back to mine. Please blast me an e-mail if interested. Kudos!
Hey there! I just wanted to ask if you ever have any problems with hackers? My last blog (wordpress) was hacked and I ended up losing several weeks of hard work due to no backup. Do you have any solutions to protect against hackers?
Também tenho o seu livro marcado para ver coisas novas no seu blog.
I’m not that much of a internet reader to be
honest but your sites really nice, keep it up! I’ll go ahead and bookmark your
website to come back in the future. All the best
Your words act as a bridge, connecting the reader to a greater understanding of the world and themselves.
You’ve woven a tapestry of insight and grace; each sentence is a thread of beauty and meaning.
Hi there!
Great post and blog thanks for sharing your with us, keep it up
Hello!
Thanks for sharing your knowledge and wisdom with us with this great job
Nosso objetivo é conectar compradores e vendedores de forma simples, rápida e segura. Você pode entrar em contato direto com o anunciante, negociar preços, agendar visitas e até solicitar uma vistoria do veículo antes da compra. seminovos em São Paulo-SP Comprar um carro usado em São Paulo-SP nunca foi tão fácil e prático.
Necrotic enteritis, a severe intestinal infection affecting poultry, can be devastating to farmers. To prevent outbreaks, it’s essential to maintain hygiene and manage bacterial threats. In a unique way, businesses involved in poultry farming can support their teams with Custom Jackets that offer both protection from environmental factors and symbolize team unity in handling such challenges.
Each sentence is like a puzzle piece fitting perfectly into a larger picture of understanding.
Your words resonate with a truth that feels universal — as though they’ve tapped into something deeply human.
Every line seems to carry a deeper meaning, as if the words are part of a larger conversation about life itself.
Your article helped me a lot, is there any more related content? Thanks!
Your article helped me a lot, is there any more related content? Thanks!
wonderful issues altogether, you simply won a new reader.What may you recommend in regards to your submit that you made some days in the past?Any certain?
BWER delivers robust, precision-engineered weighbridges to businesses across Iraq, combining state-of-the-art technology with local expertise to support infrastructure and logistics growth.
A pal stands to 1 aspect in a brown gown with a darkish mantelet.
Đừng bỏ lỡ cơ hội trải nghiệm cá cược đỉnh cao cùng Helywin. Đăng ký ngay hôm nay để nhận những ưu đãi hấp dẫn!
AlexThomas553 will bring you the most useful links currently, this place will be a valuable source of experience for you
There is definately a lot to find out about this subject. I like all the points you made
Hi to every body, it’s my first go to seeof this weblog; this web site includes amazing and really good material for readers.
Também tenho o seu livro marcado para ver coisas novas no seu blog.
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
Muito obrigado!}
že spousta z něj se objevuje na internetu bez mého souhlasu.
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
I’m not that much of a internet reader to be honest but your blogs really nice, keepit up! I’ll go ahead and bookmark your website to come back later.All the best
You are my intake, I have few web logs and infrequently run out from to post .
Great line up. We will be linking to this great article on our site. Keep up the good writing.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
In this article, we are going to explore the current actual property outlook for Wisconsin, together with current market circumstances, developments, and future predictions.
This really answered my drawback, thanks!
Oh my goodness! a great write-up dude. Many thanks Nevertheless I am experiencing problem with ur rss . Do not know why Unable to sign up for it. Can there be anyone finding identical rss issue? Anyone who knows kindly respond. Thnkx
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
Wow, this blogger is seriously impressive!
Salt trick for man growth
que eu mesmo criei ou terceirizei, mas parece que
Your style is really unique in comparison to other folks I’ve read stuff from. Many thanks for posting when you’ve got the opportunity, Guess I’ll just bookmark this page.
Grateful for the tips, thanks for writing this!
вывод из запоя на дому ростов цены forumbar.anihub.me/viewtopic.php?id=9747 .
また、会社発足当初からの役員2名は取締役兼常務執行役員となった(うち、片岡が就任する前に社長を務めていた1名は後に退任し、もう1名は後に社長に就任する渡邉廣之)。 1964年(昭和39年)11月に大神は会長となり、日本興業銀行出身の日高輝が、社長に就任。神々の詞(ことば)だとお思(おもい)。わたしはきっとお前を好(す)いている。恋に落ちた女性の態度の2つ目は、「SNSで匂わせをしたくてたまらない」です。第55条(航海中の出生)の規定は、死亡の届出にこれを準用する(戸籍法93条)。 アナログ放送では無信号状態で発生するものであり現在放送されているデジタル放送では機種により異なるが黒い画面に「この放送局は現在放送していません。
Howdy! I understand this is somewhat off-topic however I had to ask.Does operating a well-established blog such as yours take alot of work? I am brand new to operating a blog however I do write in my diary every day.I’d like to start a blog so I can share my own experience and thoughtsonline. Please let me know if you have any kind of ideas or tips for new aspiring bloggers.Appreciate it!
Today, I went to the beach with my children. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear andscreamed. There was a hermit crab inside and it pinched her ear.She never wants to go back! LoL I know this is completely off topicbut I had to tell someone!
What¦s Going down i’m new to this, I stumbled upon this I’ve discovered It positively useful and it has helped me out loads. I hope to contribute & assist other customers like its helped me. Great job.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
капельница от запоя капельница от запоя .
技能労務職員(単純労務職員)の労働関係その他身分取扱いは、原則として地方公営企業法の企業職員に関する規定が準用される(地公企労法附則第5条)ため、労働協約によって労働条件が取り決められることとなる。人事委員会を置かない地方公共団体においては、職員の採用・
I discovered your blog website on google and examine a couple of of your early posts. Continue to maintain up the excellent operate. I just further up your RSS feed to my MSN News Reader. Searching for ahead to studying more from you later on!…
Keep up the amazing work! Can’t wait to see what you have in store for us next.
We are a group of volunteers and starting a new scheme in our community. Your website provided us with valuable information to work on. You have done a formidable job and our whole community will be grateful to you.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
終盤では校長の父親が老人ホームに入居する事を桃子が勧めると聞いていた波江に激怒され反省し、「おばあちゃんと幸せになってほしい」と校長に伝えた桃子の気持ちを波江が知り関係は良好になる。恐喝の途中で久美子の登場でやむなく撤退したが、その後久美子の一言で集団での悪事から改心した高杉が「もう抜けます」と電話で伝えたことに逆上し、翌日「けじめを付けてもらうぞ」と言って仲間を連れて高杉を袋叩きにし、大事な卒業式を放り出してその高杉を取り戻しに駆け付けた3-Dの生徒たちも袋叩きにする。
Although most issues call for straightforward (although possibly difficult) answer, occasionally a problem will contain a humorous trick or twist.
Saved as a favorite, I really like your blog!
Também tenho o seu livro marcado para ver coisas novas no seu blog.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
Having read this I believed it was rather enlightening. I appreciate you finding the time and energy to put this article together. I once again find myself spending way too much time both reading and commenting. But so what, it was still worth it.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
продвижение сайтов город москва продвижение сайтов город москва .
Some genuinely interesting details you have written.Helped me a lot, just what I was looking for : D.
You made some good points there. I checked on the net to learn more about the issue and found most individuals will go along with your views on this website.
for the reason that here every material is quality based
вывод из запоя в стационаре вывод из запоя в стационаре .
“岡田 武史”.武尊勅で石楯と呼ぶ。西ノ京北部土地区画整理事業の換地処分の公告があった日は昭和25年(1950年)10月1日。京都市区の所管区域条例の一部を改正する条例(昭和25年12月1日京都市条例第64号)。京都市区の所管区域条例の一部を改正する条例(昭和29年7月29日条例第16号)。
Hello there, I discovered your web site by the use of Google while looking for a related matter,your site came up, it appears to be like good. I have bookmarked it in my google bookmarks.Hi there, simply became aware of your blog thru Google, andfound that it is really informative. I am gonna be careful for brussels.I’ll appreciate if you happen to proceed this in future.A lot of other people will probably be benefited out of yourwriting. Cheers!
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
I have to thank you for the efforts you’ve put in penning this blog. I really hope to view the same high-grade blog posts by you later on as well. In fact, your creative writing abilities has inspired me to get my own, personal blog now 😉
88 clb
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Hello, i believe that i saw you visited my site so i came to “go back the favor”.I am attempting to to find things to improve my web site!I guess its good enough to use a few of your ideas!!
Greetings from Los angeles! I’m bored to tears at work so I decided to check out yoursite on my iphone during lunch break. I really likethe knowledge you provide here and can’t wait to take a look when I gethome. I’m surprised at how quick your blog loaded on my phone.. I’m not even using WIFI, just 3G .. Anyhow,good blog!
Excellent post. I was checking constantly thisblog and I am impressed! Extremely useful info particularly the last part 🙂 I care for such info a lot.I was looking for this certain info for a very long time. Thank you and good luck.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your point. You obviously know what youre talking about, why waste your intelligence on just posting videos to your blog when you could be giving us something enlightening to read?
det. Denne side har bestemt alle de oplysninger, jeg ønskede om dette emne, og vidste ikke, hvem jeg skulle spørge. Dette er min 1. kommentar her, så jeg ville bare give en hurtig
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
çok iyi bir yer
It is appropriate time to make a few plans for the long run and it is time to be happy. I have read this publish and if I could I wish to counsel you few attention-grabbing issues or tips. Perhaps you can write next articles regarding this article. I wish to read even more issues about it!
Everything is very open with a precise explanation of the issues.It was really informative. Your site is very useful.Thanks for sharing!
Of course, what a great site and enlightening posts, I definitely will bookmark your website.Have an awsome day!
The next time I read a blog, Hopefully it does not disappoint me just as much as this particular one. After all, I know it was my choice to read, however I really thought you’d have something helpful to say. All I hear is a bunch of whining about something that you could possibly fix if you were not too busy looking for attention.
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Com tanto conteúdo e artigos, alguma vez se deparou com problemas de plágio ou violação de direitos de autor? O meu site tem muito conteúdo exclusivo que eu próprio criei ou
Com tanto conteúdo e artigos, vocês já se depararam com algum problema de plágio?
Totally exceeded my expectations! Thank you for such a fantastic service. Highly recommended!
I do agree with all the ideas you have presented in your post. They are really convincing and will definitely work. Still, the posts are very short for beginners. Could you please extend them a little from next time? Thanks for the post.
Scott & Scott 2016, p.
I love it when individuals get together and share ideas. Great blog, stick with it!
然(しか)るに文武の業は自ら士の常職となりて、平生は廟堂に坐して政權を持し、一旦緩急あれば兵を執り亂を撥する等、獨(ひと)り士族の責(せめ)のみに委(まか)し、國家の興亡安危に至りては平民(へいみん)曾(かつ)て與(あづ)かり知らず、坐視傍觀の勢となり行きしは、全く中古封建制度の弊にして、貴重靈物の責(せめ)を私(わたくし)し、賤民をして愈賤劣ならしむる所以也。 そのため、西洋文明の積極的導入(「文明開化」)を推進し、地租改正や殖産興業で経済力をつけ(=富国)、徴兵制や軍制改革により軍備を増強(=強兵)することで国家の自立維持を図った。
You are so cool! I don’t suppose I’ve read something like that before. So great to discover someone with some unique thoughts on this subject matter. Seriously.. thanks for starting this up. This site is one thing that’s needed on the web, someone with a bit of originality.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
You are my breathing in, I have few blogs and occasionally run out from to post : (.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Do you mind if I quote a few of your articles as long as I provide credit and sources back to your webpage? My blog is in the exact same niche as yours and my users would definitely benefit from some of the information you present here. Please let me know if this okay with you. Cheers!
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
I’m not that much of a internet reader to be honest but yoursites really nice, keep it up! I’ll go ahead and bookmark your site to come back later.Cheers
State development planning or national planning entails macroeconomic policies and financial planning conducted by governments to stabilize the market or promote economic growth in market-based economies.
Some truly interesting information, well written and broadly user genial.
Hiya, I am really glad I’ve found this info. Nowadays bloggers publish just about gossips and internet and this is actually annoying. A good website with interesting content, that is what I need. Thank you for keeping this website, I will be visiting it. Do you do newsletters? Cant find it.
En iyi Online Casino
WONDERFUL Post.thanks for share..more wait .. …
Usually, there are two ways to pay your property taxes: rolled into your monthly mortgage payment or on to your native tax office.
Howdy! Do you know if they make any plugins to protect against hackers?I’m kinda paranoid about losing everything I’ve workedhard on. Any recommendations?
Tonerin is a natural supplement crafted to bolster the cardiovascular system by promoting healthy blood pressure levels and enhancing circulation. Infused with potent ingredients like hawthorn and garlic, it strengthens blood vessels and supports heart function, offering a gentle alternative for those aiming to improve their heart health without pharmaceutical intervention.
Potential sources are corn and switchgrass.
This site was… how do you say it? Relevant!! Finally I’ve found something that helped me. Cheers!
This site was… how do you say it? Relevant!! Finally I’ve found something which helped me. Thanks a lot.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
This is a topic that is close to my heart… Many thanks! Where can I find the contact details for questions?
Hey There. I found your blog using msn. This is a very well written article. I’ll make sure to bookmark it and return to read more of your useful info. Thanks for the post. I will certainly return.
Greetings! Very helpful advice within this post! It is the little changes that produce the biggest changes. Thanks for sharing!
Com tanto conteúdo e artigos, vocês já se depararam com algum problema de plágio?
landuse Funny Porn lancdcuse.Z19bcqjzQ3B
Everything is very open with a precise description of the issues. It was definitely informative. Your site is useful. Thanks for sharing.
Great post! We are linking to this particularly great article on our site.Keep up the great writing.
pB61rG1PeEf
Your trust in us is our utmost importance. Therefore, we operatewith absolute transparency and focus on results.Rest easy of recovering your QIWI wallet balancewith our specialized assistance.
sex nhật hiếp dâm trẻ em ấu dâm buôn bán vũ khí ma túy bán súng sextoy chơi đĩ sex bạo lực sex học đường tội phạm tình dục chơi les đĩ đực người mẫu bán dâm
Why people still use to read news papers when in this technological world everything is presented on web?
Hello i am kavin, its my first time to commenting anywhere, when i read this post
i thought i could also create comment due to this sensible article.
Your style is really unique compared to other people I’ve read stuff from. I appreciate you for posting when you’ve got the opportunity, Guess I’ll just bookmark this site.
Hi, Neat post. There is a problem with your website in internet explorer, would test this… IE still is the market leader and a huge portion of people will miss your excellent writing because of this problem.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Wow, this article is amazing! Your writing style is so engaging and kept me hooked from start to finish. The topic is so relevant and helpful. Keep creating!
I could not refrain from commenting. Very well written.
e dizer que gosto muito de ler os vossos blogues.
Howdy, I do believe your site might be having web browser compatibility problems. Whenever I take a look at your site in Safari, it looks fine however when opening in IE, it’s got some overlapping issues. I merely wanted to provide you with a quick heads up! Aside from that, great site.
It is not simply an inquiry into how doubtless you’re to sacrifice plush motels for hostel beds.
díky tomuto nádhernému čtení! Rozhodně se mi líbil každý kousek z toho a já
Peppermint or menthol preparations are to start with irreplaceable in native anaesthetics, as well as for the relief of inflammatory processes that are so frequent among the beginner-yogis.
I always emailed this webpage post page to all my contacts, for the reason that
if like to read it then my contacts will too.
I love your blog.. very nice colors & theme. Did you create this website yourself or did you hire someone to do it for you? Plz respond as I’m looking to design my own blog and would like to know where u got this from. kudos
díky tomuto nádhernému čtení! Rozhodně se mi líbil každý kousek z toho a já
Thanks for your marvelous posting! I genuinely enjoyed reading it, you might be a great author.I will make certain to bookmark your blog and will eventually come back from now on. I want to encourage that you continue your great writing, have a nice day!
Great post. I was checking constantly this blog and I am impressed! Extremely useful info specially the last part 🙂 I care for such info much. I was looking for this certain information for a very long time. Thank you and best of luck.
That is a good tip especially to those new to the blogosphere. Simple but very precise information… Many thanks for sharing this one. A must read article!
BOM86 là cổng game đổi thưởng đẳng cấp nhất hiện nay. Tại đây mọi người sẽ được trải nghiệm các game cá cược hấp dẫn như casino online , game bài và bắn cá.
Very nice article. I certainly love this website. Thanks!
This is a topic which is near to my heart… Cheers! Where can I find the contact details for questions?
This is a great tip particularly to those new to the blogosphere. Short but very accurate info… Appreciate your sharing this one. A must read post!
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Great article! We are linking to this particularly great article on our site. Keep up the great writing.
Very good info. Lucky me I came across your website by accident (stumbleupon). I have saved as a favorite for later.
Your style is unique compared to other people I have read stuff from. Many thanks for posting when you have the opportunity, Guess I will just bookmark this blog.
Does your website have a contact page? I’m havingtrouble locating it but, I’d like to send you an e-mail.I’ve got some suggestions for your blog you might be interested in hearing.Either way, great blog and I look forward to seeing it expand over time.
Your point of view caught my eye and was very interesting. Thanks. I have a question for you.
Lovely just what I was searching for.Thanks to the author for taking his clock time on this one.
enten oprettet mig selv eller outsourcet, men det ser ud til
Supporters are invited to return down early for tonight’s match at the J. Davidson Stadium between Altrincham and Kidderminster Harriers as the Television screens within the bar of the Neighborhood Sports Corridor will likely be showing, stay, the England v Kazakhstan below-21s’ match.
Sweet blog! I found it while browsing on Yahoo News. Do you have any tips on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Cheers
Everything is very open with a very clear explanation of the challenges. It was definitely informative. Your website is extremely helpful. Thanks for sharing!
We can’t allow an impasse over lengthy-term fiscal challenges to distract us from what the middle class wants right now.
Join Sex The most efficient choice for anyone looking for a fast and online solution.
You have made some decent points there. I checked on the net to find out more about the issue and found most individuals will go along with your views on this website.
I want to to thank you for this fantastic read!! I certainly enjoyed every bit of it. I have got you bookmarked to check out new stuff you post…
Sure, you can. Any good hand sander can be utilized, though the job will take considerably longer, and most have no kind of dust management.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
I’d like to thank you for the efforts you’ve put in writing this site. I really hope to see the same high-grade blog posts from you in the future as well. In truth, your creative writing abilities has inspired me to get my own blog now 😉
I’d like to thank you for the efforts you’ve put in penning this site. I really hope to see the same high-grade content by you later on as well. In fact, your creative writing abilities has encouraged me to get my own, personal site now 😉
Your writing style is so engaging and easy to follow I find myself reading through each post without even realizing I’ve reached the end
Hi there, I discovered your web site by means of Google while searching for a similar subject, your site got here up, it appears to be like great. I’ve bookmarked it in my google bookmarks.
Can I just say what a relief to find someone who actually knows what theyre talking about on the internet. You definitely know how to bring an issue to light and make it important. More people need to read this and understand this side of the story. I cant believe youre not more popular because you definitely have the gift.
hello!,I like your writing so much! share we communicate more about your post on AOL? I need a specialist on this area to solve my problem. May be that’s you! Looking forward to see you.
gruppe? Der er mange mennesker, som jeg tror virkelig ville
Confused about how to go about the recovery of your QIWI wallet funds?Our professional advisors are on standby around the clock to guide you through the procedure and answer any concerns you have.Working with our team, you’re choosing a reliable partner in financial recovery.
左様(さう)君のやうに無理なことを為(し)なくツても好からう。保険期間中の総填補限度額の設定 – 1度に被害者が多数生じたり、損害額が多額となる恐れがあるリスクを対象とする保険の場合は、保険技術上、1事故あたりの填補限度額の設定に加えて、保険期間中の総填補限度額(Aggregate Limit)が設定されることがあるが、この保険がその1つである(例えば、施設所有管理者賠償責任保険や請負業者賠償責任保険には、保険期間中の総填補限度額の設定はない)。桜蘭学院理事長。
Your article helped me a lot, is there any more related content? Thanks!
I wanted to write a simple remark to be able to express gratitude to you for these remarkable tips and hints you are giving at this website. My extensive internet research has finally been paid with professional tips to share with my great friends. I ‘d assume that most of us website visitors actually are unequivocally lucky to exist in a really good site with many lovely individuals with very beneficial suggestions. I feel pretty happy to have used the web site and look forward to many more fabulous times reading here. Thanks a lot once more for all the details.
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
This page definitely has all of the information I wanted about this subject and didn’t know who to ask.
However plenty of other companies need a bit of the tablet pie — and so they see a possibility in providing decrease-priced models far cheaper than the iPad.
You have made some good points there. I looked on the netfor more information about the issue and found most people will goalong with your views on this site.
Wow, fantastic blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your site is magnificent, let alone the content!
BOM86 là cổng game đổi thưởng đẳng cấp nhất hiện nay. Tại đây mọi người sẽ được trải nghiệm các game cá cược hấp dẫn như casino online , game bài và bắn cá.
I have recently started a site, the info you offer on this website has helped me tremendously. Thanks for all of your time & work.
Great info. Lucky me I came across your blog by chance (stumbleupon). I have book-marked it for later!
1win. 1win2.md .
Děkuji|Ahoj všem, obsah, který je na této stránce k dispozici.
Would you be all in favour of exchanging hyperlinks?
Can I simply say what a comfort to uncover an individual who genuinely knows what they are talking about over the internet. You definitely know how to bring a problem to light and make it important. More and more people should read this and understand this side of the story. I can’t believe you are not more popular because you surely have the gift.
Very well written information. It will be beneficial to anyone who usess it, including yours truly :). Keep up the good work – can’r wait to read more posts.
I am constantly impressed by the depth and detail in your posts You have a gift for making complex topics easily understandable
I simply could not depart your web site prior to suggestingthat I actually enjoyed the standard information a person provide for your visitors?Is going to be again often to investigate cross-check new posts
Its like you read my mind! You appear to know so much about this, like you wrote the book in it or something. I think that you can do with some pics to drive the message home a bit, but instead of that, this is magnificent blog. A great read. I’ll definitely be back.
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Introducing to you the most prestigious online entertainment address today. Visit now to experience now!
This website was… how do you say it? Relevant!! Finally I’ve found something which helped me. Thanks a lot.
I’m gone to say to my little brother, that he should also visit this website on regular basis to
take updated from latest news update.
Good day! Do you know if they make any plugins to safeguard against hackers? I’m kinda paranoid about losing everything I’ve worked hard on. Any tips?
I very delighted to find this site on bing, just what I was searching for : D as well saved to my bookmarks.
Undeniably believe that which you stated. Your favorite reason seemed to be on the internet the easiest thing to be aware of. I say to you, I definitely get irked while people think about worries that they plainly don’t know about. You managed to hit the nail upon the top and also defined out the whole thing without having side-effects , people can take a signal. Will probably be back to get more. Thanks
Unique viewpoints, because who needs echo chambers?
Great content! Super high-quality! Keep it up! 🙂
この時代からマケドニア王国が隆盛を迎えるまでこの地域がギリシャ史の中核を成すのであるが、これは栽培物にオリーブ、ブドウが導入されたことが考えられている。新井政美『トルコ近現代史: イスラム国家から国民国家へ』みすず書房、2001年(改訂版2008年)。宮城美里町北浦・ バイドゥ株式会社 (2022年3月22日).2022年3月26日閲覧。日本テレビ. 2022年10月12日時点のオリジナルよりアーカイブ。 メディア芸術カレントコンテンツ (2020年10月15日).2022年11月27日閲覧。 13 May 2020. 2020年5月16日閲覧。
Way cool! Some very valid points! I appreciate you penning this post plus the rest of the website is extremely good.
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
10月にハワイ大学での日本美術のシンポジウムを現地の研究者と共同で企画し、研究発表を行った。同月16日に都内の病院へ入院、19日には手術を受けることとなった。包帯を替えてくれたのも、術後の経過を見てくれたのも本当に助かりました!祖父:吉田茂(第45・皇室においては、清子内親王(黒田清子)以降9人連続の女子(内親王4名・
I don’t think the title of your article matches the content lol. Just kidding, mainly because I had some doubts after reading the article.
This is really interesting, You are a very skilled blogger.
I’ve joined your feed and look forward to seeking more of your great post.
Also, I’ve shared your site in my social networks!
I like it when people get together and share opinions. Great
site, stick with it!
Together with every thing which seems to be building within this subject material, all your opinions are fairly radical. However, I am sorry, because I do not subscribe to your entire strategy, all be it radical none the less. It would seem to everybody that your remarks are actually not completely validated and in actuality you are your self not wholly confident of your assertion. In any event I did take pleasure in examining it.
In this grand pattern of things you’ll receive an A+ for effort and hard work. Where exactly you lost us ended up being on all the facts. You know, it is said, the devil is in the details… And it could not be much more true in this article. Having said that, permit me inform you what did deliver the results. The writing is definitely pretty convincing and this is possibly the reason why I am making the effort to opine. I do not make it a regular habit of doing that. 2nd, while I can easily notice the jumps in reason you come up with, I am not really sure of how you seem to unite your details which in turn produce the actual conclusion. For right now I will yield to your position however trust in the near future you link the facts much better.
Hi there, just became aware of your blog through Google, and found that it istruly informative. I’m going to watch out for brussels.I will appreciate if you continue this in future.Numerous people will be benefited from your writing.Cheers!
I am perpetually thought about this, thanks for posting.
Your article helped me a lot, is there any more related content? Thanks!
https://russiamarkets.to/
https://russiamarkets.to/
https://briansclub.bz/
Do you mind if I quote a couple of your articles as long as I provide credit and sources back to your blog? My website is in the exact same niche as yours and my visitors would certainly benefit from some of the information you provide here. Please let me know if this alright with you. Cheers!
Kender du nogen metoder, der kan hjælpe med at forhindre, at indholdet bliver stjålet? Det ville jeg sætte stor pris på.
muito dele está a aparecer em toda a Internet sem o meu acordo.
gruppe? Der er mange mennesker, som jeg tror virkelig ville
Hi there, i read your blog occasionally and i own a similar one and i was just curious if you get a lot of spam remarks? If so how do you reduce it, any plugin or anything you can suggest? I get so much lately it’s driving me insane so any help is very much appreciated.
I was suggested this blog by my cousin. I am not sure whether this post is written by him as no one else know such detailed about my difficulty. You’re incredible! Thanks!
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
See the highlights rhino
Good shout.
webside er virkelig bemærkelsesværdig for folks oplevelse, godt,
gruppe? Der er mange mennesker, som jeg tror virkelig ville
værdsætter dit indhold. Lad mig venligst vide det.
enten oprettet mig selv eller outsourcet, men det ser ud til
Kan du anbefale andre blogs / websteder / fora, der beskæftiger sig med de samme emner?
díky tomuto nádhernému čtení! Rozhodně se mi líbil každý kousek z toho a já
gruppe? Der er mange mennesker, som jeg tror virkelig ville
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
Nice
skupině? Je tu spousta lidí, o kterých si myslím, že by se opravdu
where to buy thca area 52
2 gram carts area 52
cbd gummies for sleep area 52
live resin carts area 52
full spectrum cbd gummies area 52
liquid diamonds area 52
where to buy shrooms area 52
indica gummies area 52
live resin gummies area 52
best disposable vaporizers area 52
infused pre rolls area 52
sativa gummies area 52
thca diamonds area 52
thca gummies area 52
mood thc gummies area 52
live resin area 52
best pre rolls area 52
best sativa thc carts area 52
thc gummies for pain area 52
thc tinctures area 52
thc pen area 52
thc oil area 52
1 gram carts area 52
DP
JH
I have been browsing online more than 3 hours today, yet I never found any interesting article like yours. It is pretty worth enough for me. In my view, if all website owners and bloggers made good content as you did, the internet will be a lot more useful than ever before.
apreciariam o seu conteúdo. Por favor, me avise.
Almost all of whatever you articulate is astonishingly appropriate and it makes me wonder why I hadn’t looked at this with this light before. This particular piece truly did switch the light on for me as far as this topic goes. However at this time there is actually one particular point I am not necessarily too cozy with and while I try to reconcile that with the central idea of the position, permit me observe just what all the rest of the visitors have to point out.Very well done.
buď vytvořil sám, nebo zadal externí firmě, ale vypadá to.
Its like you read my mind! You seem to know so much about this, like you wrote the book in it or something. I think that you can do with a few pics to drive the message home a little bit, but instead of that, this is excellent blog. An excellent read. I will definitely be back.
Appreciating the time and effort you put into your website and in depth information you provide. It’s awesome to come across a blog every once in a while that isn’t the same outdated rehashed information. Fantastic read! I’ve bookmarked your site and I’m adding your RSS feeds to my Google account.
Tak Hej der til alle, det indhold, der findes på denne
fortsæt med at guide andre. Jeg var meget glad for at afdække dette websted. Jeg er nødt til at takke dig for din tid
Esta página tem definitivamente toda a informação que eu queria sobre este assunto e não sabia a quem perguntar. Este é o meu primeiro comentário aqui, então eu só queria dar um rápido
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
meget af det dukker op overalt på internettet uden min aftale.
Com tanto conteúdo e artigos, alguma vez se deparou com problemas de plágio ou violação de direitos de autor? O meu site tem muito conteúdo exclusivo que eu próprio criei ou
grupo do facebook? Há muitas pessoas que eu acho que iriam realmente
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
nenarazili jste někdy na problémy s plagorismem nebo porušováním autorských práv? Moje webové stránky mají spoustu unikátního obsahu, který jsem vytvořil.
Nice
snow caps thca area 52
thc gummies for anxiety area 52
live rosin gummies area 52
thc microdose gummies area 52
thc sleep gummies area 52
distillate carts area 52
disposable weed pen area 52
thc gummies
thcv gummies area 52
hybrid weed vaporizer area 52
best thca flower area 52
hybrid gummies area 52
thca disposable area 52
liquid thc area 52
ZA
Fiquei muito feliz em descobrir este site. Preciso de agradecer pelo vosso tempo
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
råb ud og sig, at jeg virkelig nyder at læse gennem dine blogindlæg.
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
meget af det dukker op overalt på internettet uden min aftale.
enten oprettet mig selv eller outsourcet, men det ser ud til
I apologise, but, in my opinion, you are not right. I can prove it.
værdsætter dit indhold. Lad mig venligst vide det.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
pokračujte v pěkné práci, kolegové.|Když máte tolik obsahu a článků, děláte to?
apreciariam o seu conteúdo. Por favor, me avise.
fortsæt det gode arbejde stipendiater. Med at have så meget indhold og artikler gør du det
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
الاستمرار في توجيه الآخرين.|Ahoj, věřím, že je to vynikající blog. Narazil jsem na něj;
https://the.hosting/
|Hello to all, for the reason that I am actually keen of
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
webside er virkelig bemærkelsesværdig for folks oplevelse, godt,
meget af det dukker op overalt på internettet uden min aftale.
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
Também tenho o seu livro marcado para ver coisas novas no seu blog.
مرحبًا، أعتقد أن هذه مدونة ممتازة. لقد عثرت عليها بالصدفة ;
buď vytvořil sám, nebo zadal externí firmě, ale vypadá to.
Kan du anbefale andre blogs / websteder / fora, der beskæftiger sig med de samme emner?
grupo do facebook? Há muitas pessoas que eu acho que iriam realmente
I was very happy to uncover this web site. I need to to thank you for your time due to this wonderful read!! I definitely really liked every little bit of it and i also have you book-marked to look at new things on your blog.
Znáte nějaké metody, které by pomohly omezit krádeže obsahu? Rozhodně bych ocenil
I will revisit once again since i have book-marked it. Money and freedom is the best way to change, may you be rich and continue to guide others.
apreciariam o seu conteúdo. Por favor, me avise.
https://ping.space/
skupině? Je tu spousta lidí, o kterých si myslím, že by se opravdu
Tak skal du have!|Olá, creio que este é um excelente blogue. Tropecei nele;
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
Também tenho o seu livro marcado para ver coisas novas no seu blog.
vykřiknout a říct, že mě opravdu baví číst vaše příspěvky na blogu.
O conteúdo existente nesta página é realmente notável para a experiência das pessoas,
Hello there, just became aware of your blog through Google, and found that it
is really informative. I’m going to watch out for brussels.
I will be grateful if you continue this in future.
Numerous people will be benefited from your writing.
Cheers!
Kan du anbefale andre blogs / websteder / fora, der beskæftiger sig med de samme emner?
apreciariam o seu conteúdo. Por favor, me avise.
devido a esta maravilhosa leitura!!! O que é que eu acho?
|Tato stránka má rozhodně všechny informace, které jsem o tomto tématu chtěl a nevěděl jsem, koho se zeptat.|Dobrý den! Tohle je můj 1. komentář tady, takže jsem chtěl jen dát rychlý
https://ufo.hosting/cms-hosting/hosting-cms-prestashop
) Vou voltar a visitá-lo uma vez que o marquei no livro. O dinheiro e a liberdade são a melhor forma de mudar, que sejas rico e continues a orientar os outros.
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
devido a esta maravilhosa leitura!!! O que é que eu acho?
Hi there! I’m at work surfing around your blog from my new iphone 4! Just wanted to say I love reading through your blog and look forward to all your posts! Carry on the outstanding work!
webové stránky jsou opravdu pozoruhodné pro lidi zkušenosti, dobře,
I believe one of your ads triggered my internet browser to resize, you might want to put that on your blacklist.
Hi there! I know this is kind of off topic but I was wondering if you knew where I could locate a captcha plugin for my comment form? I’m using the same blog platform as yours and I’m having problems finding one? Thanks a lot!
Díky moc!|Hej, jeg synes, dette er en fremragende blog. Jeg snublede over det;
My developer is trying to convince me to move to .net from PHP. I have always disliked the idea because of the expenses. But he’s tryiong none the less. I’ve been using WordPress on a number of websites for about a year and am anxious about switching to another platform. I have heard excellent things about blogengine.net. Is there a way I can transfer all my wordpress content into it? Any kind of help would be really appreciated!
také jsem si vás poznamenal, abych se podíval na nové věci na vašem blogu.|Hej! Vadilo by vám, kdybych sdílel váš blog s mým facebookem.
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
Thanks for ones marvelous posting! I definitely enjoyed reading it, you happen to be a great author.I will make sure to bookmark your blog and will often come back later on. I want to encourage you to continue your great job, have a nice morning!
We are a group of volunteers and starting a new scheme in our community. Your website provided us with valuable information to work on. You have done an impressive job and our entire community will be thankful to you.
Hi, i read your blog from time to time and i own a similar one and i was just wondering if you get a lot of spam comments? If so how do you stop it, any plugin or anything you can advise? I get so much lately it’s driving me insane so any support is very much appreciated.
råb ud og sig, at jeg virkelig nyder at læse gennem dine blogindlæg.
Greetings! This is my first comment here so I just wanted to give a quick shout out and say I genuinely enjoy reading through your blog posts. Can you suggest any other blogs/websites/forums that go over the same subjects? Thanks for your time!
Thanks, I have recently been searching for info about this subject matter for ages and yours is the best I’ve discovered so far.
Your article helped me a lot, is there any more related content? Thanks!
I have been browsing online greater than 3 hours nowadays, yet I never found any interesting article like yours. It’s beautiful price enough for me. Personally, if all webmasters and bloggers made excellent content material as you probably did, the web might be much more helpful than ever before.
tenerife yacht charters
I have been surfing online more than three hours nowadays, yet I never discovered any interesting article like yours. It’s pretty price enough for me. In my opinion, if all site owners and bloggers made good content material as you probably did, the web will likely be much more helpful than ever before.
I have been surfing online greater than three hours these days, yet I by no means found any interesting article like yours. It’s beautiful worth enough for me. Personally, if all website owners and bloggers made good content material as you did, the web will likely be a lot more helpful than ever before.
Как только начал играть — сразу почувствовал волну. Если ищешь что-то настоящее, что держит от начала до конца — начни с https://vodka-registration.site. Можно играть хоть с утра до ночи. Тут главное — динамика и отдача. Промокоды придают игре вкус. Игры продуманы до деталей. Бонусы не просто на словах — они реально работают. Выплаты приходят стабильно, это главное. Кто не рискует — тот не выигрывает. А здесь рискуют с удовольствием.
Не люблю банальные казино с кричащими баннерами и обещаниями «1000% за регистрацию». Я искал место, где можно просто спокойно поиграть, не чувствуя себя лохом под прицелом алгоритма. Оказалось, что всё, чего мне не хватало — это регистрация в Vodka Casino. Без пафоса, без давления: минималистично, честно и с достойным выбором автоматов. Выигрыш не гарантирован, но когда он приходит — чувствуешь, что заслужил. Особенно понравилось, что можно играть с телефона без скачивания — один вечер на даче, и у меня уже был плюс к отпускному бюджету. Главное — не гнаться за крупняком, а ловить момент, когда комбинации складываются не только на экране, но и в голове.
Hello very nice blog!! Guy .. Excellent .. Superb ..
I’ll bookmark your site and take the feeds also? I’m happy to search out a lot of helpful info right here
within the publish, we need work out more strategies in this regard, thanks for sharing.
. . . . .
Не каждый день удаётся сыграть так, чтобы потом вспоминать часами. Для меня отправной точкой стало скачать приложение Vodka Casino. Интерфейс не важен, если внутри огонь. Бонусы не просто на словах — они реально работают. Промокоды придают игре вкус. Тут главное — динамика и отдача. Азарт здесь настоящий — как в офлайн клубе.
Когда хочется расслабиться, не всегда подходят сериалы или YouTube. Мне лично помогает хорошее казино, и https://vodka-registration.site в этом плане стал открытием. Всё просто: выбрал игру, поставил ставку, пошёл процесс. И это затягивает. Особенно если на счету приятный бонус за регистрацию. Даже если проиграл — получаешь кэшбэк. Никакой агрессии со стороны платформы, только честный подход. Промокоды приходят по делу, а не «на всякий случай». Игры оптимизированы под телефон, ничего не лагает. А зеркало — как спасательный круг в море блокировок. Работает всегда, когда нужно.
Всё началось с обычного вечера, когда я решил попробовать что-то новое и скачать приложение для игры. скачать Vodka Casino оказалось не просто удачной идеей, а настоящим открытием. Установилось быстро, авторизация заняла пару секунд, и вот я уже на экране с десятками слотов и разделом ставок на спорт. Это приложение не просто функциональное — оно будто живёт и дышит, мгновенно реагируя на каждый мой клик. Даже когда интернет нестабилен, всё продолжает работать плавно и без подвисаний. Особенно радует система бонусов — каждый день есть что-то новое: кэшбэк, фриспины, промокоды и прочие приятности, которые делают игру по-настоящему захватывающей. Отдельно хочу отметить поддержку: живой чат решает всё в течение пары минут, без шаблонных отписок и «перезагрузите устройство». Такое отношение вдохновляет возвращаться снова и снова. Слоты с живыми дилерами, турниры с реальными соперниками, моментальные выплаты на карту или криптокошелёк — всё это работает на ура. Мобильное приложение не просто удобно, оно делает азарт доступным в любой момент: в метро, в очереди, дома на диване. Это не просто игра, это образ жизни.
https://auctionwheels.info/cars/pontiac/models/wave/pagination/start
) سأعيد زيارتها مرة أخرى لأنني قمت بوضع علامة كتاب عليها. المال والحرية هي أفضل طريقة للتغيير، أتمنى أن تكون غنيًا و
på grund af denne vidunderlige læsning !!! Jeg kunne bestemt virkelig godt lide hver eneste lille smule af det, og jeg
at web, except I know I am getting familiarity all the time by reading thes pleasant posts.|Fantastic post. I will also be handling some of these problems.|Hello, I think this is a great blog. I happened onto it;) I have bookmarked it and will check it out again. The best way to change is via wealth and independence. May you prosper and never stop mentoring others.|I was overjoyed to find this website. I must express my gratitude for your time because this was an amazing read! I thoroughly enjoyed reading it, and I’ve bookmarked your blog so I can check out fresh content in the future.|Hi there! If I shared your blog with my Facebook group, would that be okay? I believe there are a lot of people who would truly value your article.|منشور رائع. سأتعامل مع بعض هذه|
que eu mesmo criei ou terceirizei, mas parece que
information.|My family members every time say that I am killing my time here
det. Denne side har bestemt alle de oplysninger, jeg ønskede om dette emne, og vidste ikke, hvem jeg skulle spørge. Dette er min 1. kommentar her, så jeg ville bare give en hurtig
) Jeg vil besøge igen, da jeg har bogmærket det. Penge og frihed er den bedste måde at ændre sig på, må du være rig og
It contains fastidious material.|I think the admin of this website is actually working hard in favor of his site,
Audio started playing as soon as I opened up this blog, so irritating!
Together with every little thing that appears to be building within this particular subject matter, all your viewpoints tend to be somewhat exciting. On the other hand, I appologize, but I do not give credence to your entire idea, all be it exciting none the less. It appears to us that your remarks are generally not totally justified and in actuality you are your self not even wholly certain of the argument. In any event I did take pleasure in looking at it.
Hey I am so delighted I found your website, I really found you by accident, while I was browsing on Digg for something else, Anyhow I am here now and would just like to say many thanks for a fantastic post and a all round enjoyable blog (I also love the theme/design), I don’t have time to browse it all at the minute but I have saved it and also added your RSS feeds, so when I have time I will be back to read a great deal more, Please do keep up the superb work.
pokračovat v tom, abyste vedli ostatní.|Byl jsem velmi šťastný, že jsem objevil tuto webovou stránku. Musím vám poděkovat za váš čas
Wonderful goods from you, man. I’ve understand your stuff previous to and you are just too excellent. I really like what you have acquired here, really like what you are saying and the way in which you say it. You make it entertaining and you still care for to keep it wise. I can’t wait to read much more from you. This is actually a terrific website.
råb ud og sig, at jeg virkelig nyder at læse gennem dine blogindlæg.
Hello this is somewhat of off topic but I was wanting to know if blogs use WYSIWYG editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding expertise so I wanted to get guidance from someone with experience. Any help would be enormously appreciated!
Também tenho o seu livro marcado para ver coisas novas no seu blog.
Hey there I am so grateful I found your blog, I really found you by accident, while I was browsing on Askjeeve for something else, Regardless I am here now and would just like to say many thanks for a tremendous post and a all round interesting blog (I also love the theme/design), I don’t have time to go through it all at the moment but I have bookmarked it and also added your RSS feeds, so when I have time I will be back to read a lot more, Please do keep up the great work.
I absolutely love your blog and find the majority of your post’s to be exactly I’m looking for. Do you offer guest writers to write content for you personally? I wouldn’t mind producing a post or elaborating on many of the subjects you write concerning here. Again, awesome web log!